Article Text

Statistics from Altmetric.com
A strong association between birdshot chorioretinopathy and HLA-A29 expression has been well established.1 In fact, some have suggested that HLA-A29 expression is essential to make the diagnosis of birdshot chorioretinopathy. Such a strong association makes accurate HLA-A29 subtyping quite important in patients suspected of having this entity. Herein, we describe two patients with birdshot chorioretinopathy in whom initial testing for HLA-A29 expression using antibody-based methods was negative and subsequent testing using more sensitive and specific PCR-based techniques was positive.
Case 1
A 45-year-old Caucasian man with a history of psoriatic skin lesions presented with worsening vision, floaters, and nyctalopia affecting both eyes for 2 months prior to presentation. Best corrected visual acuity was 20/25 in each eye. Intraocular pressures were normal bilaterally. Anterior segment examination revealed 1+ cell and flare in the anterior chamber and 2+ cell in the anterior vitreous in each eye. Posterior segment examination revealed diffuse vitreous inflammation, mild disc oedema, diffusely dilated retinal veins and multiple yellow-white choroidal lesions in the mid- and far-periphery of each eye (fig 1). Fluorescein angiography showed leakage from the optic disc and retinal vessels bilaterally. Extensive laboratory evaluation, including serum FTA-ABS and RPR titres, serum ACE and lysozyme levels, chest x ray, and antibody testing for HLA-A29 expression, were unrevealing. Clinical suspicion of birdshot chorioretinopathy remained high, however, so repeat testing for HLA-A29 expression using PCR-based techniques was performed and found to be positive.
Case 2
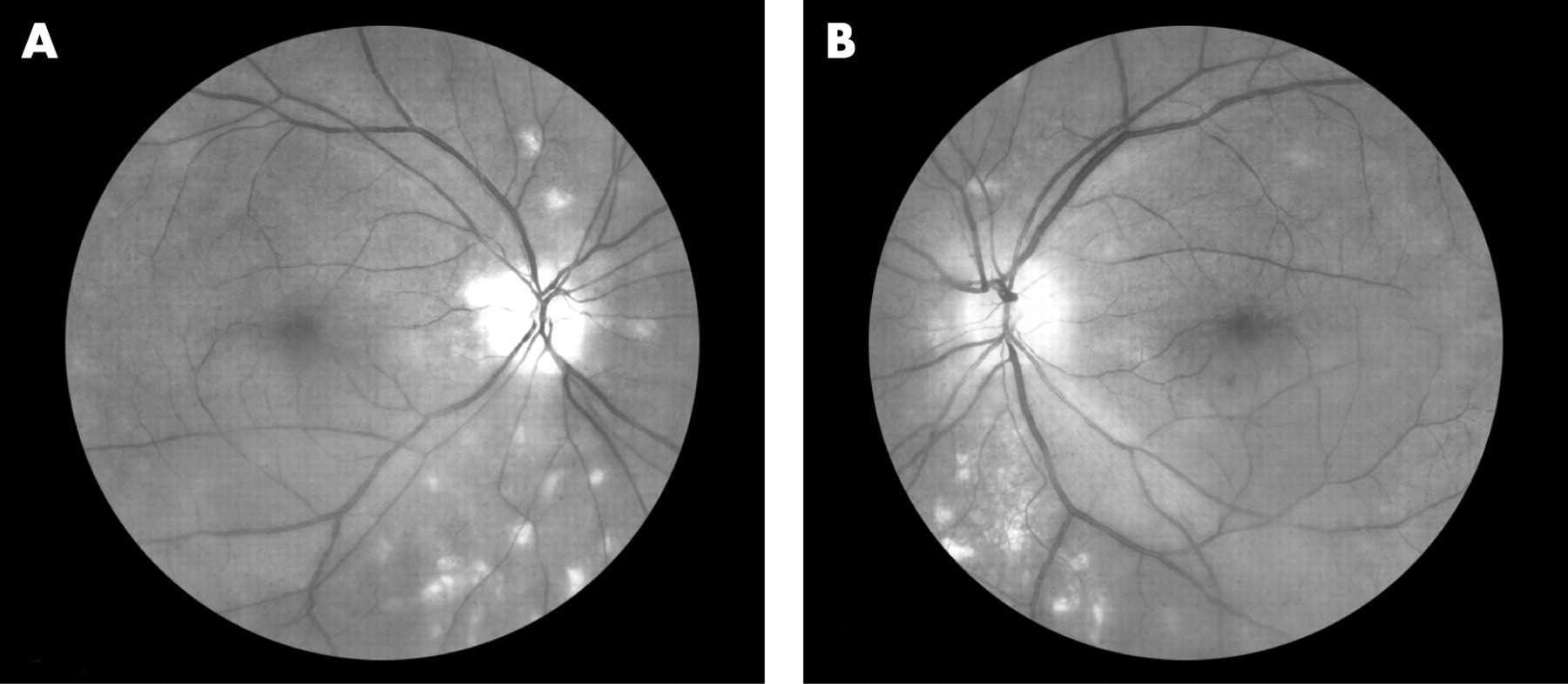
A 39-year-old Caucasian woman was seen with best-corrected visual acuity 20/25+1 in the right eye and 20/30+2 in the left eye. Intraocular pressures were normal bilaterally. Anterior segment examination was unremarkable. Posterior segment examination revealed scattered vitreous cells and multiple yellow-white choroidal lesions in the mid- and far-periphery of each eye (fig 2). Extensive laboratory evaluation, including serum FTA-ABS and RPR titres, serum ACE and lysozyme levels, and chest x ray were unrevealing. Antibody-based HLA-A29 testing was negative on two separate occasions. Clinical suspicion of birdshot chorioretinopathy remained high, however, so PCR-based testing for the HLA-A29 expression was requested and found to be positive.

{kind=link}
{kind=link}
Although the precise pathogenesis of birdshot chorioretinopathy is unknown, the vast majority of patients express HLA-A29, and the presence of this class I antigen confers a markedly elevated relative risk for developing the disease.1 2 In addition, HLA-A29 transgenic mice have been shown to develop a spontaneous retinopathy similar to birdshot chorioretinopathy.3 Among patients with this entity, almost all express subtype 2 of the HLA-A29 antigen.1 2 Accordingly, in populations where the prevalence of HLA-A29 subtype 2 expression is low, birdshot chorioretinopathy is correspondingly less frequent.4 Accurate testing for HLA-A29 expression is therefore essential for establishing an accurate diagnosis and treatment plan in patients with clinical features consistent with this disease.
Historically, HLA testing was performed using antibody-based methods. PCR-based techniques for HLA subtyping have emerged more recently, however, and have been shown to be more sensitive and specific than antibody-based approaches, including testing for HLA-A29 expression.5 6 While our report represents the first description of false negative antibody-based HLA-A29 testing, similarly false negative outcomes have been reported in patients tested for HLA-B27 expression.7 Such findings suggest that PCR-based subtyping should be considered in patients with characteristic birdshot chorioretinopathy, particularly when antibody-based methods produce an unexpected negative result.
Footnotes
Funding: Supported in part by The San Francisco Retinal Foundation and The Pacific Vision Foundation.
Competing interests: None declared.
Patient consent: Obtained.