Article Text

Statistics from Altmetric.com
- Choroidal macrovessel
- indocyanine green angiography
- retinal macrovessel
- spectral domain optical coherence tomography
- choroid
- eye (globe)
- anatomy
- imaging
- medical education
Case report
A 42-year-old white man presented for a routine evaluation. The patient had a history of travelling through developing countries. There was no history of trauma. Best corrected visual acuity was 20/20 in the right eye and 20/100 in the left eye. Dilated fundus examination of the right eye revealed a serpiginoid atrophic lesion in the temporal macula and multifocal chorioretinitic spots without any sign of acute inflammation. The lesion extended from the temporal paramacular area to the temporal periphery (figure 1). An optic nerve coloboma was observed in the left eye accounting for its diminished vision.

Fundus colour photograph of the right eye showing a serpiginoid-like atrophic tract corresponding to a choroidal macrovessel. The choroidal macrovessel extends from the periphery to the temporal macula with foveal avascular zone sparing.
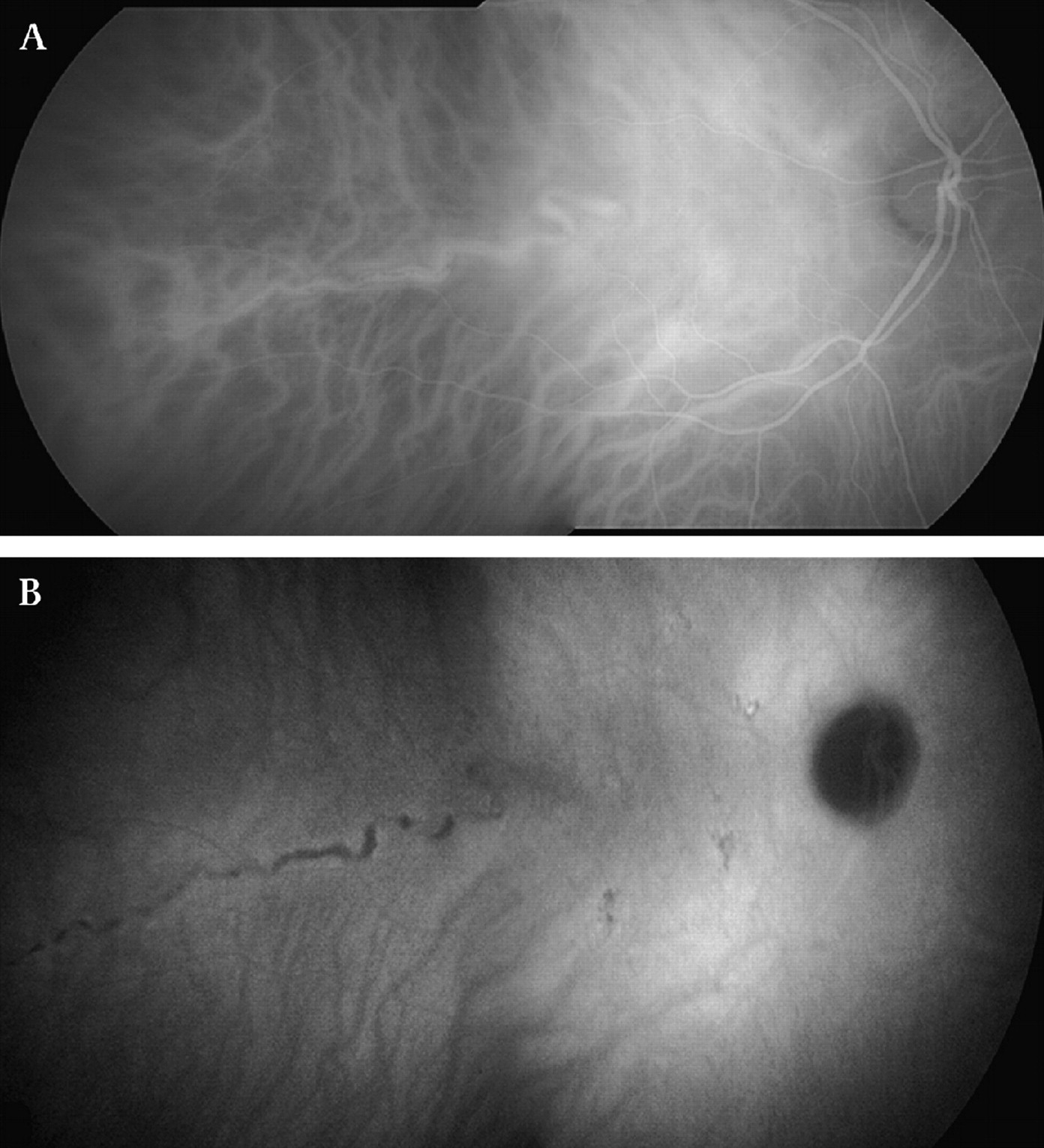
Fluorescein angiography (FA) of the right eye demonstrated normal filling and laminar flow in the both retinal arteries and veins. The filling pattern of the choroidal vessels, including the suspected lesion, was normal and occurred before the perfusion of the retinal vasculature. The lesion was hyperfluorescent consistent with perfusion of a choroidal vessel. No evidence of arteriovenous anastomosis, capillary nonperfusion, or late leakage was detected. Indocyanine green angiography (ICG) showed perfusion of the lesion with the ICG dye and hypofluorescence of the presumed vascular abnormality in the late phase of the exam (figure 2).

Indocyanine green angiography reveals a normal fluorescence in the early phase (A) with a hypofluorescence in the macrovessel tract in the late phase of the exam (B). There is no evidence of arteriovenous anastomosis, capillary nonperfusion or late leakage.
Further evaluation of the right eye using spectral domain optical coherence tomography (SD-OCT; Heidelberg Spectralis, Heidelberg Engineering GmbH, Heidelberg, Germany) was performed with scans transecting the course of the lesion in the macula. There was hyperreflectivity in the choroid corresponding to the edge of the lesion with associated posterior shadowing (figure 3). We also measured the diameter of the presumed choroidal anomalous vessel and the corresponding choroidal vessel in the fellow eye, using a caliper available in the IMAGENET program software. The diameters of the presumed choroidal anomalous vessel and the corresponding choroidal vessel in the fellow eye were 326 and 90 μm, respectively.

{kind=link}
{kind=link}
{kind=link}
(A) Spectral domain optical coherence tomography scan with the corresponding infra-red imaging (B) shows hyperreflectivity in the choroid corresponding to the course of the macrovessel with associated posterior shadowing (arrow).
Discussion
Different nematodes such as Oedemagena tarandi (Ophthalmomyiasis) and Alaria americanus have been implicated in subretinal atrophic and cicatricial tracts in the fundus.1–4 A americanus is a short and thick nematode that can leave ruggedly irregular subretinal tract with possible secondary exudative changes. Ophthalmomyiasis is accidentally transmitted to humans by a warble fly (O tarandi) and can also cause subretinal tracts characterised by a criss-crossing configuration. Also, gnathostomiasis and diffuse unilateral subacute neuroretinitis can rarely produce subretinal tracts.5 6 Other intraocular nematode disease such as cysticercosis and angiostrongyliasis can produce inflammatory chorioretinal scars and optic disc hemorrhages, but not subretinal tracts. The serpiginoid nature of the lesion in this case was suspicious for a subretinal nematode tract, in particular a filarial organism. Such nematodes are known to produce long, tortuous, atrophic and/or cicatricial tracts at the level of the retinal pigment epithelium from the worm's entry site to its point of burrowing into the choroid to induce an exudative reaction.7 8 The patient's history of travelling through developing countries heightened the suspicion of a nematode as a possible explanation for the lesion.
In addition to a potential subretinal nematode, an anomalous posterior ciliary vessel was also considered as an explanation for the lesion. Normal short posterior ciliary arteries differ distinctly from the lesion. These arteries enter the eye near the disc or in the central macula as small caliber vessels which perfuse the posterior fundus.9 The temporal long posterior ciliary artery enters the eye near the optic nerve to course along the horizontal meridian, first briefly through the sclera and eventually into the outer choroid to provide the circulation for the anterior uvea.9 In our case, the lesion was first seen just temporal to the fovea to course within a tortuous configuration in the inner choroid, only to descend posteriorly out of sight into outer uveal scleral area. FA, ICG and SD-OCT were useful imaging modalities to study the lesion. In the case of a nematode tract which has affected the pigment epithelium, there is either early window defect or late staining of sclera from elements of fibrovascular tissue within the streak in the late stages of the angiogram.10 ICG was helpful in analysing the lesion further, as it showed vascular perfusion coincidental with the arrival of the dye and its bioconjugate molecules in the choroid in the early stage of the study and a silhouette of the lesion in the late stage as the dye left the circulation, except for leakage into the extrachoroidal space. Further confirmation of the vascular nature of the lesion was provided by SD-OCT to delineate a tubular structure in the inner choroid, in contact with the retinal pigment epithelium.
While the vascular nature of the lesion could be established, no normal choroidal vessel is known to satisfy all of the criteria evident clinically, angiographically, and tomographically. The best explanation to reconcile these peculiar anatomical inconsistencies in the nature of the lesion is an anomalous choroidal macrovessel. Congenital retinal macrovessels are known to occur not uncommonly in the fundus.11–14 They are often larger and more tortuous than normal retinal vessels, and they perfuse a geographic zone which is larger than the distribution of normal vessels. Single congenital retinal macrovessels may perfuse a half or two-thirds of the fundus, crossing the horizontal raphe. Angiography of retinal macrovessels demonstrates a prolonged transient time.15 These vessels also have a predilection for vascular occlusive disease.16 Although they do not normally stain with FA, there may be associated ischaemia, leakage, remodelling, and even preretinal neovascularization in the event of a trombotic occlusion.17 18 In our case, the peculiar segmental anomalous vascular lesion in the choroid showed no staining within its wall with either fluorescein or indocyanine-green; it demonstrated a choroidal-pigment epithelial proximity, with a tubular elevation of the retinal pigment epithelium and choroidal layers with point to point correlation on the SD-OCT. This elevation included both the inner segments/outer segments junction of the photoreceptors and the external limiting membrane. This peculiar pattern was present in the fundus only at the site of the clinically visible large and tortuous segment of the choroidal vascular lesion. The diameter of the presumed anomalous vessel was larger than the normal diameter of the choroidal vessel which varies between 20 and 100 μm.19
Our presumption is that this case represents a choroidal macrovessel. To our knowledge, this is the first choroidal macrovessel reported in the ophthalmic literature. Since there is no available clinico-histopathological correlation of such a vessel, further observation and clinical pathological studies are needed to confirm this impression. Identification and longitudinal examinations to follow the natural course of this anomalous vessel are needed to determine its predilection for pathological changes. In the meantime, the use of multi-modal imaging is useful in differentiating such a lesion from nematode tract, particularly in endemic areas where such infestations are more common.
References
Footnotes
Funding This work was supported by the LuEsther T. Mertz Retina Research Center, Manhattan Eye, Ear, and Throat Hospital, and The Macula Foundation Inc.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.