Article Text

Statistics from Altmetric.com
Punctate inner choroidopathy is an idiopathic inflammatory ocular disorder characteristically seen in young myopic women. Visual prognosis is generally good but sight threatening choroidal neovascularisation may develop in up to 40% patients.1 We discuss verteporfin photodynamic therapy in subfoveal choroidal neovascularisation secondary to punctate inner choroidopathy that failed to respond to oral corticosteroids and had poor results with submacular surgery in the contralateral eye.
Case report
A 40 year old white female patient with punctate inner choroidopathy was referred to our macular clinic with rapidly deteriorating vision in her left eye secondary to a subfoveal choroidal neovascularisation. She had a history of poor vision in the right eye following submacular surgery to remove a subfoveal choroidal neovascular membrane. Best corrected vision was hand movements in the right eye and 6/18 in the left eye. The logMAR acuity in the left eye was 0.46 (38 letters misread). The anterior segments and intraocular pressures were normal. Both fundi showed characteristic multiple pigmented atrophic scars in the posterior pole and mid-periphery in the absence of vitreous cells. There was a macular scar in the right eye (Fig 1). In the left eye there was an elevated grey lesion with subretinal fluid and intraretinal haemorrhages (Fig 2A). Fluorescein angiography confirmed a predominantly classic subfoveal choroidal neovascular membrane (Fig 2B and C). Argon laser photocoagulation was contraindicated because of the subfoveal location. Despite a 4 week course of oral prednisolone (40 mg a day for 1 week then reduced by 10 mg every week) the vision in the patient’s only useful eye continued to worsen. The patient refused submacular surgery because of the poor postoperative result in her right eye. Photodynamic therapy was offered as a treatment option.

Right eye. The photograph shows the large central macular scar with retinal pigment hypertrophy and atrophy following surgical removal of a choroidal neovascularisation. Smaller circumscribed pigmented atrophic scars characteristic of punctate inner choroidopathy are seen in the mid-periphery.
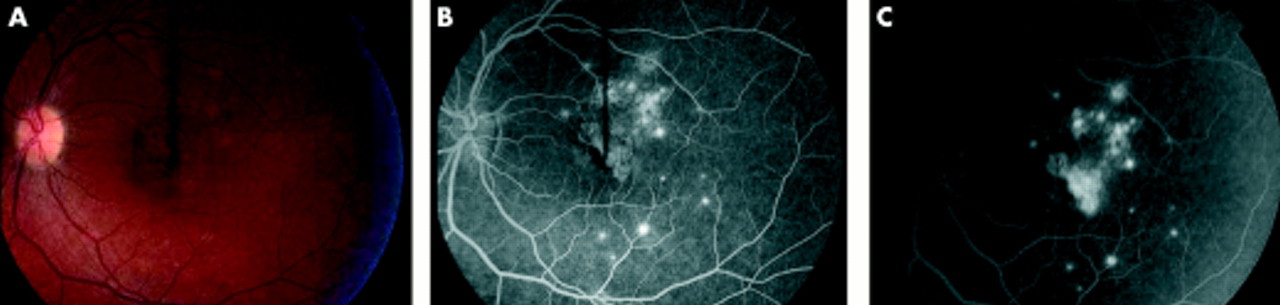
Left eye at presentation. (A) The colour photograph shows a grey elevated subfoveal lesion associated with intraretinal haemorrhages and subretinal fluid and surrounding smaller atrophic pigmented lesions characteristic of punctate inner choroidopathy. (B) The arteriovenous phase of the fluorescein angiogram at 28.2 seconds shows a hyperfluorescent subfoveal choroidal neovascularisation with a typical lacy pattern and smaller punctate hyperfluorescent lesions of punctate inner choroidopathy. The area of blocked fluorescence is consistent with the intraretinal haemorrhage. (C) The late arteriovenous phase of the fluorescein angiogram at 2.09 minutes shows increased hyperfluorescence and active leakage of dye from the subfoveal choroidal neovascularisation.
After obtaining informed consent we performed five sessions of photodynamic therapy at 3 monthly intervals according to a standard protocol. Baseline and 3 monthly post-treatment logMAR visual acuities were recorded and clinical and angiographic assessment was performed. After 15 months the Snellen acuity in her left eye has stabilised at 6/18 and her logMAR acuity is 0.2 (25 letters misread). She has gained eight letters on the logMAR chart and subjectively there is less distortion. Clinically, there is resolution of the subretinal fluid and intraretinal haemorrhages and formation of a flat scar-like lesion (Fig 3A). Angiographically, despite some early leakage, the findings are consistent with reduced activity and fibrosis of the choroidal neovascularisation (Fig 3B and C). An indocyanine green angiography confirmed the findings of the fluorescein angiography and excluded the presence of choroidal feeder vessels that could lead to a recurrence of the neovascularisation (Fig 4).

Left eye after five verteporfin photodynamic sessions. (A) The colour photograph shows a flat subfoveal scar-like lesion with resolution of subretinal fluid and intraretinal haemorrhages. (B) The arteriovenous phase of the fluorescein angiogram at 21 seconds shows some early hyperfluorescence with reduced activity and size of the lesion. (C) The late arteriovenous phase of the fluorescein angiogram at 1.05 minute shows mainly staining of fibrosis and no active leakage.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
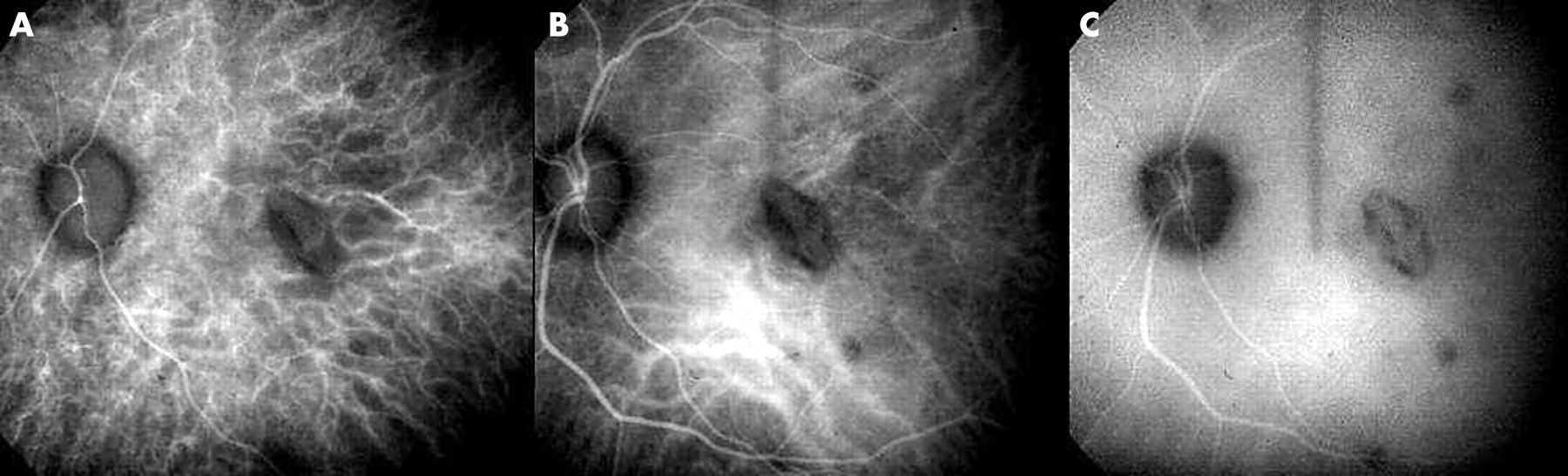
(A–C) Indocyanine green angiography of the left eye after five verteporfin photodynamic sessions at 11 seconds, 55.2 seconds, and 9.35 minutes showing no active choroidal neovascularisation and no feeder vessels.
Comment
Punctate inner choroidopathy is an idiopathic inflammatory disorder that usually occurs in young, myopic women.2 Both eyes are commonly affected. Symptoms include blurred or distorted vision, light flashes, or paracentral scotomas.2 The acute, multiple, yellow-white lesions of the inner choroid and retina of the posterior pole evolve into atrophic pigmented scars.2 Vitritis and anterior uveitis are absent.2 Visual prognosis is good in most patients and significant visual loss is usually due to formation of choroidal neovascularisation.1 Choroidal neovascularisation if smaller than 100 μm in diameter may resolve spontaneously.1 However, subfoveal choroidal neovascularisation occurs in 40% of the patients.1 Argon laser photocoagulation is contraindicated for subfoveal lesions.1 Although good results have been reported with 1 mg/kg per day of oral prednisolone,3 the response to oral steroids is variable if more than 200 μm in diameter.1 Submacular surgery has shown promising results but recurrence is common.4
Photodynamic therapy using verteporfin is safe and effective for subfoveal choroidal neovascularisation in age related macular degeneration and high myopia.5,6 The verteporfin guidelines suggested photodynamic therapy for other aetiologies if outcome without treatment was likely to be poor.7 Preliminary success in ocular histoplasmosis syndrome, angioid streaks, idiopathic and other conditions has been reported.8–15 The recommended protocol for treatment included clinical and angiographic review every 3 months.5,7 Retreatment was indicated if there was any fluorescein leakage from the choroidal neovascularisation.5,7 Retreatment was deferred if the visual acuity remained stable or improved and the lesion fulfilled all the following criteria7: (1) minimal or no subretinal fluid on biomicroscopic examination; (2) flat scar-like appearance; (3) minimal fluorescein leakage without progression beyond the boundaries of the previous treatment or involvement of the fovea.
Photodynamic therapy in this case of subfoveal choroidal neovascularisation secondary to punctate inner choroidopathy was indicated after a poor surgical result in the first eye and the deterioration of vision in the fellow eye despite oral corticosteroid treatment. Five treatment sessions over 15 months produced subjective and visual (logMAR) improvement. Clinically there was resolution of intraretinal haemorrhages and subretinal fluid with formation of a flat scar-like lesion. The angiogram confirmed a stable lesion with minimal fluorescein leakage, no progression beyond the boundaries of the previous treatment and staining of the scar tissue. This case demonstrates that verteporfin photodynamic therapy may be a useful treatment option in choroidal neovascularisation due to punctate inner choroidopathy. Further studies are needed to confirm and support this observation.