Article Text

Statistics from Altmetric.com
Intrastromal corneal ring segments (ICRS) are polymethyl methylacrylate implants placed in the mid-peripheral cornea without destruction or removal of tissue. The displacement of corneal lamellae produces shortening of the central corneal arc length and flattening of the central cornea.1 It is for this reason that there has been interest in the use of ICRS for the treatment of myopia and, more recently, keratoconus.
The benefits of ICRS over some other refractive procedures include reversibility or potential for adjustment; sparing of the central cornea; maintenance of the positive asphericity of the cornea and, in the case of keratoconus, potential to delay or obviate the need for corneal transplantation.2 However, as with all biomedical implants, infection remains a risk.
We report a case of microbial keratitis following ICRS implantation.
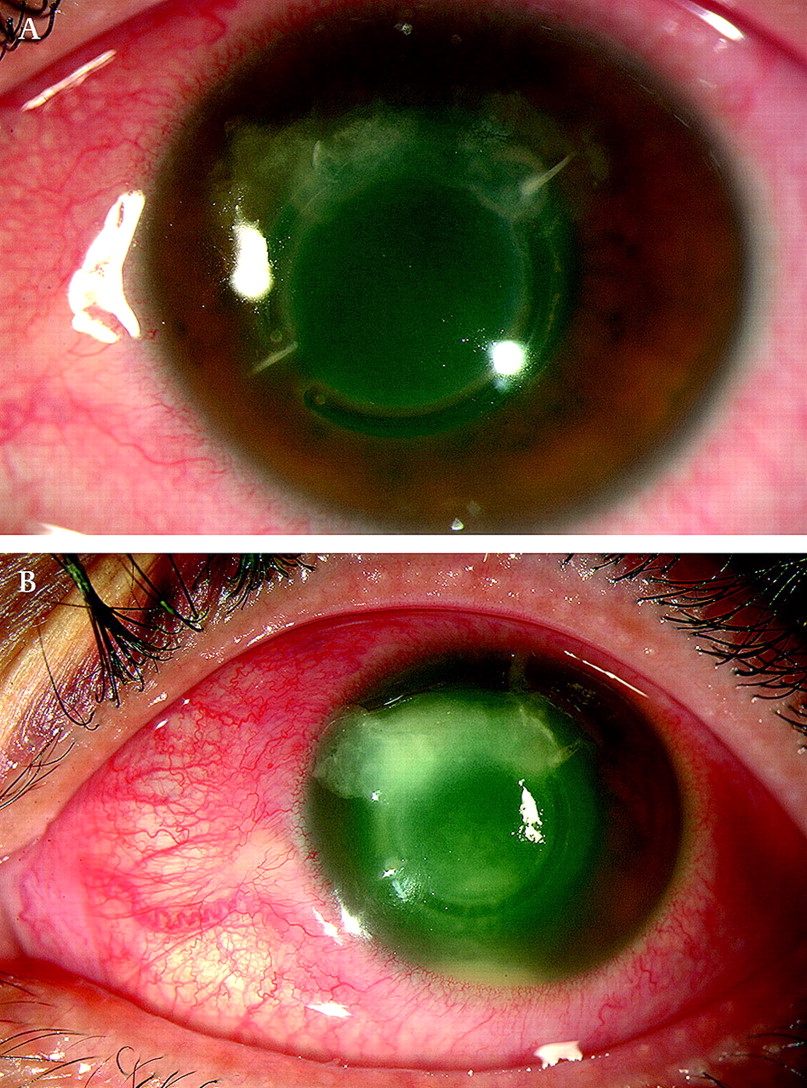
A 40-year-old healthy woman presented 3 months after bilateral 160° Ferrara rings insertion for keratoconus. She complained of worsening pain in her left eye over the past 24 h. Best corrected visual acuity (BCVA) was 1/60 on presentation. Slit lamp examination revealed deep infiltrates around the superior ring segment, microcystic corneal oedema, diffuse punctuate epitheliopathy and anterior chamber inflammation. (figure 1A) There was no hypopyon. The fellow eye revealed ICRS segments with no other pathology. Intraocular pressure was 38 mmHg in the left eye and 18 mmHg in the right eye.
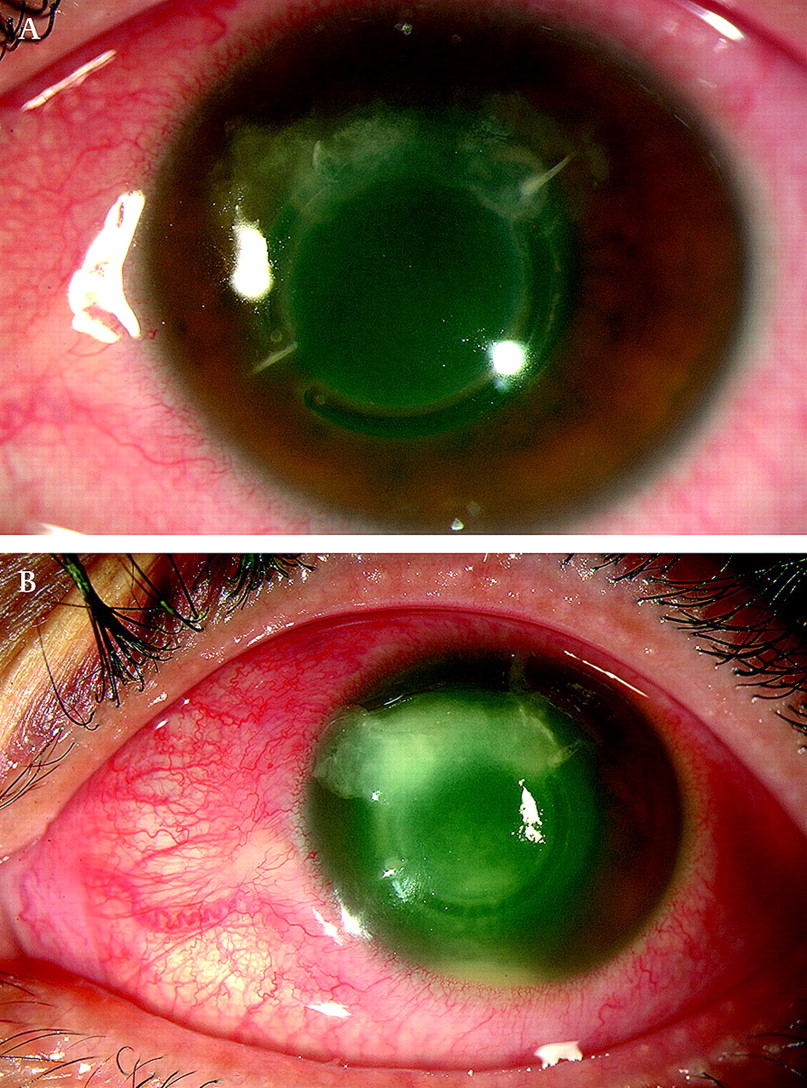
(A) Slit lamp photograph of the left eye on presentation, showing infiltrates around superior Ferrara ring segment. (B) Slit lamp photograph of the left eye 24 h after presentation, with worsening of infiltrates and hypopyon.
Previous records revealed that the pre-operative uncorrected visual acuity was count fingers at 2 m in both eyes. Pre-operative refraction was −9.0/−5.75×30 and −3.50/−6.25×110 in the right and left eyes, respectively. Keratometry measurements were 45.09/50.5 and 44.13/51.0 in the right and left eyes, respectively, pre-operatively. At 1 month postoperatively, BCVA was 20/60 in both eyes, with a refraction of −1.75/3.00×150 and −4.00/−2.75×20 in the right and left eyes, respectively.
On presentation, corneal scrapings were obtained for microscopy including Gram and Giemsa stains and bacterial and fungal cultures and sensitivities. The patient was hospitalised, and intensive treatment was commenced with topical ofloxacin hydrochloride 0.3% every hour, homatropine 2% three times a day, timolol 0.5% twice a day and brimonidine 0.02% twice a day.
The initial culture revealed Staphylococcus epidermidis. Within 24 h of admission, the patient had worsened with increase in the size of the infiltrates and a fresh hypopyon (figure 1B). Treatment was changed to fortified topical cefazolin 5% and tobramycin 1.3%. The condition continued to worsen, and the ICRS were removed 48 h after admission through the original entry points and sent for culture. The superior ICRS had partially extruded, and the channel was opened to the corneal surface. Repeat corneal scrapings were taken. Each channel was irrigated with vancomycin 5%.
S epidermidis was again cultured and was found to be resistant to cefazolin and ofloxacin. Treatment was changed to hourly vancomycin 5% eye drops, and the hourly tobramycin 1.3% was continued.
The patient's symptoms improved and the hypopyon resolved following implant removal. The patient was discharged on topical vancomycin, tobramycin and fluorometholone.
At last review, approximately 12 weeks following the initial presentation, BCVA was 1/60 in the left eye. There was corneal stromal haze at the site of the implant, and the overlying epithelial defect had resolved (figure 2). The patient is awaiting a penetrating keratoplasty.

{kind=link}
{kind=link}
Slit lamp photograph of the left eye 12 weeks following removal of Ferrara Rings, showing corneal stromal haze and no epithelial defect.
Questions
What are the complications associated with the implantation of ICRS?
What are the likely causes of microbial keratitis in a case with ICRS?
How would you manage a case of microbial keratitis after ICRS implantation?
See page 1555 for answer
Answers
From questions on page 1541
The implantation of ICRS may be associated with complications like extrusion of the rings, persistent incisional gap, corneal stromal thinning, sterile infiltration and microbial keratitis.
Several factors may contribute to the development of infection after placement of ICRS. There may be a possible breakdown of the overlying epithelium or extrusion of the ring from the channel. Presence of a suture at the end of the channel and use of multiple incisions are the other factors that may contribute to the occurrence of microbial keratitis in cases with ICRS.
The initial management involves microbiological analysis of corneal scrapings obtained from the site of infection and intensive topical antibiotic therapy. Conservative management rarely works if the infection spreads to the bed of the channel and explantation of the segment is almost always mandatory.
Discussion
Infection following implantation of ICRS is a serious complication and can occur many months after the initial procedure.3–9 The literature contains several case reports and series of infectious keratitis following ICRS implantation.10–14 In all the reported cases, the time from surgery to the development of infectious keratitis ranged from <1 week to 22 months,10 and in several cases, therapeutic penetrating keratoplasty was required for control of the infection.10
The risk of acquiring infection in the operated eye is usually associated with corneal epithelial breakdown, presence of a loose suture, use of multiple incisions or a wound gape. The extrusion of intracorneal ring segment and subsequent corneal infection may be related to the superficial placement of the ring during initial surgery. More recently, Ferrara rings are being implanted using a single incision in order to eliminate problems associated with the use of multiple incisions.
Once infection develops, it is imperative to evaluate the clinical condition. If there is no wound gape or extrusion of ICRS, conservative management with intensive antibiotic therapy may be tried. If there is involvement of the bed of the channel or extensive microbial keratitis with or without extrusion of the segment, explantation of the segment and collection of microbiological specimen are recommended.15 The channel should be drained with antibiotics and left open. In our case, the microbial keratitis could not be resolved with intensive antibiotic treatment. The infection progressed to the bed of the channel within first 24 h along with the appearance of a fresh hypopyon. We, therefore, decided to explant the ICRS to prevent corneal perforation. There was a rapid resolution of the infiltrates following the removal of the ICRS implants.
Our case highlights the risk of occurrence of microbial keratitis after implantation of ICRS. Once infection occurs, the choice of treatment modality depends on the extent and severity of involvement.
References
Footnotes
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.