Article Text

Statistics from Altmetric.com
Introduction
Choroidal blood drainage is highly varied.1 Generally, each of the four quadrants of the eye converge to form a large dilated vascular channel called the ampulla. The ampulla is about 1.5–2 mm wide and up to 5 mm long; it drains into the vortex veins.2 The main drainage route is through 6–8 vortex veins, which perforate the sclera at the equator. Another route is defined as the posterior route, where the blood drains out either through the choriovaginal veins, which penetrate the sclera near the optic nerve on the macular side, or through the macular vortex veins, which penetrate the sclera under the macula.3 (figure 1A)

(A) A scheme to demonstrate the choroidal drainage. Green vessels show the peripheral drainage. Blue and red vessels show the rare peripheral drainage. Blue vessels demonstrate choriovaginal vessels, red vessels demonstrate the macular vortex veins. Black arrows show the direction of the flow and the drainage point. (B) Fundus photography of the left eye. (C) Indocyanine green angiography of the left eye while normal breathing. (D) Indocyanine green angiography while performing Valsalva manoeuvre. The difference is not noticeable.
Unusual dilation of the peripherally routed vortex veins at the site of ampulla has been reported a number of times.4–8 Choroidal varices are generally asymptomatic and often found coincidentally in patients of middle age.4 The aetiology is unknown, but greater haemodynamic stress in the macular region, hypertension and aging are considered to be responsible.5 Extreme gaze is reported to result in expansion of the varix at the venous vortex ampulla.6
Case report
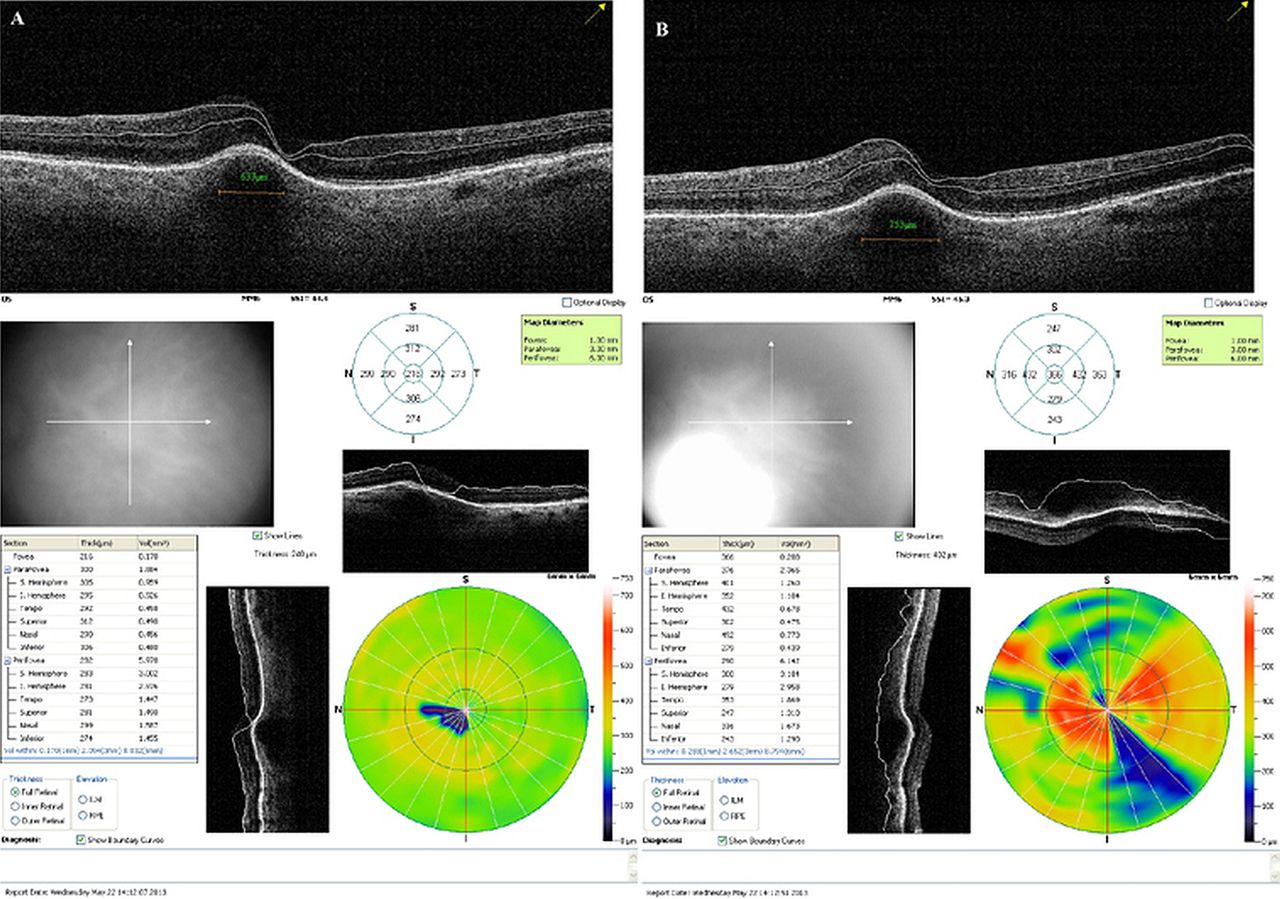
A 45-year-old man presented to our facility with a 2-year history of intermittent blurred vision in his left eye, especially while performing heavy lifting tasks. He described mainly metamorphopsia, but at initial examination his best-corrected visual acuity was 20/20 in both eyes. Slit lamp microscopy showed that he had tortuous conjunctival veins and dilated examination of the fundus revealed a retinal elevation along a choroidal varix, without remarkable colour, that began in the posterior pole, going beneath the macula with a downward and temporal course. It was about 9 mm long and 2 mm wide (figure 1B). His vision was not altered, and consequently only a follow-up was suggested, but our patient was insistent on asking why his vision was decreasing while performing heavy lifting tasks. Therefore, he was called back the next day in order to investigate the issue and we noticed that the vision in his left eye dropped to 16/20 after he performed a Valsalva manoeuvre. The Valsalva manoeuvre increased the intraocular pressure from 19 to 23 mm Hg. Our patient had no palpable thrill on the left eye. The best explanation was that the choroidal varix was expanding during the Valsalva manoeuvre and elevating the macula. Fluorescein angiography, indocyanine green angiography (figure 1C,D), MRI, colour Doppler imaging and optical coherence tomography (OCT) were all performed. The MRI results showed no evidence of caroticocavernous fistula, or any other pathology. Colour Doppler imaging of the ophthalmic, central retinal and posterior ciliary arteries was used to measure the peak systolic blood flow velocities and the vascular resistance index within these vessels, but these were found to be within the normal ranges in both eyes and there was no significant difference following Valsalva manoeuvres. The expansion of the varicose vortex vein with the Valsalva manoeuvre could only be demonstrated statically with the OCT (figure 2A,B).

{kind=link}
{kind=link}
(A) Left eye, optical coherence tomography (OCT) showing the choroidal varix and the central retinal thickness (B) The dilation of the choroidal vessel and the thickening in the central retina while performing Valsalva manoeuvre is demonstrable. Note that the OCT on the right side was taken only seconds later.
Questions
-
Does the choroid have an autoregulatory capacity during alterations in transmural pressure?
-
What effects does the Valsalva manoeuvre have on the eye?
-
What is the best method for imaging a choroidal varix?
FOR ANSWERS SEE 148
Answers (FOR QUESTIONS SEE 138)
-
Does the choroid have an autoregulatory capacity during alterations in transmural pressure?
Traditionally the choroid is known to have no autoregulation that responds to vascular pressure.9 The myogenic theory assumes that the smooth muscles of the choroidal vasculature respond to transmural pressure, which is shown in a study on the choroidal circulation of rabbits.10 A recent clinical study also confirms that choroid shows some autoregulatory capacity.9
-
What effects does the Valsalva manoeuvre have on the eye?
The Valsalva manoeuvre is performed by exhaling against a closed glottis. The increased abdominal and intrathoracic pressure decreases the venous return and increases the pressure in the head and the neck. It is reported that the Valsalva manoeuvre increases the intraocular pressure transiently, but that the thickness of the choroid does not change.11 Nevertheless, it has been reported to cause preretinal haemorrhage, known as Valsalva retinopathy, as well as macular haemorrhage, suprachoroidal haemorrhage, Purtscher's-like retinopathy and retinal vein occlusion. To the best of our knowledge, there have been no previous report of a similar reversible visual disturbance due to a change in the shape of the macula when the Valsalva manoeuvre is performed.
-
What is the best method for imaging a choroidal varix?
In this case, the haemodynamics of the choroidal varix were difficult to demonstrate using either MRI or colour Doppler imaging, but indocyanine green angiography and OCT were better choices for measuring the width of the retinal vessels and demonstrating the dilation.
Discussion
In the present case, the unusually dilated part of the venula was not just at the ampulla: the entire venula was dilated. Also, the venula had a peripheral drainage and was longer than 9 mm and about 2 mm wide (figure 1).
Polypoidal choroidal vasculopathy (PCV) has been found to be associated with vascular engorgement and dilation.12 However, our patient's diagnosis was not compatible with the criteria for PCV as it is defined in a recent major review because he had no focal areas of hyperfluorescence arising from the choroidal circulation after injection of indocyanine green.13
This unique case highlights the autoregulatory capacity of the choroid and may also shed light on the way choroidal vasculature responds to Valsalva manoeuvre.
Footnotes
-
Contributors EC contributed in analysis, interpretation of data and in concept and design of the study. ME, VD and KM contributed in acquisition and interpretation of the data. OŞ and OÇ contributed in the revision of the study and final approval of the version to be published.
-
Competing interests All authors have completed the ICMJE uniform disclosure form at http://www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years; no other relationships or activities that could appear to have influenced the submitted work.
-
Patient consent Obtained.
-
Ethics approval The patient has approved this report.
-
Provenance and peer review Not commissioned; externally peer reviewed.