Article Text

Statistics from Altmetric.com
The epidemic of blindness from retinopathy of prematurity (ROP) is spreading and is now affecting countries in Asia and the Pacific region as well as Latin America and Eastern Europe. An estimated 32 300 infants became blind or visually impaired from ROP in the year 2010, with the largest number being in the East and Southeast Asia and Pacific region.1 The spread of the epidemic is due to several factors, the most important being the welcomed expansion of services for sick and preterm newborns in emerging economies, particularly in the large populations in Asia and the Pacific, which has led to greater survival of preterm infants. Unfortunately, policies and programmes for the detection and treatment of ROP have not always kept pace with the expansion of neonatal care.
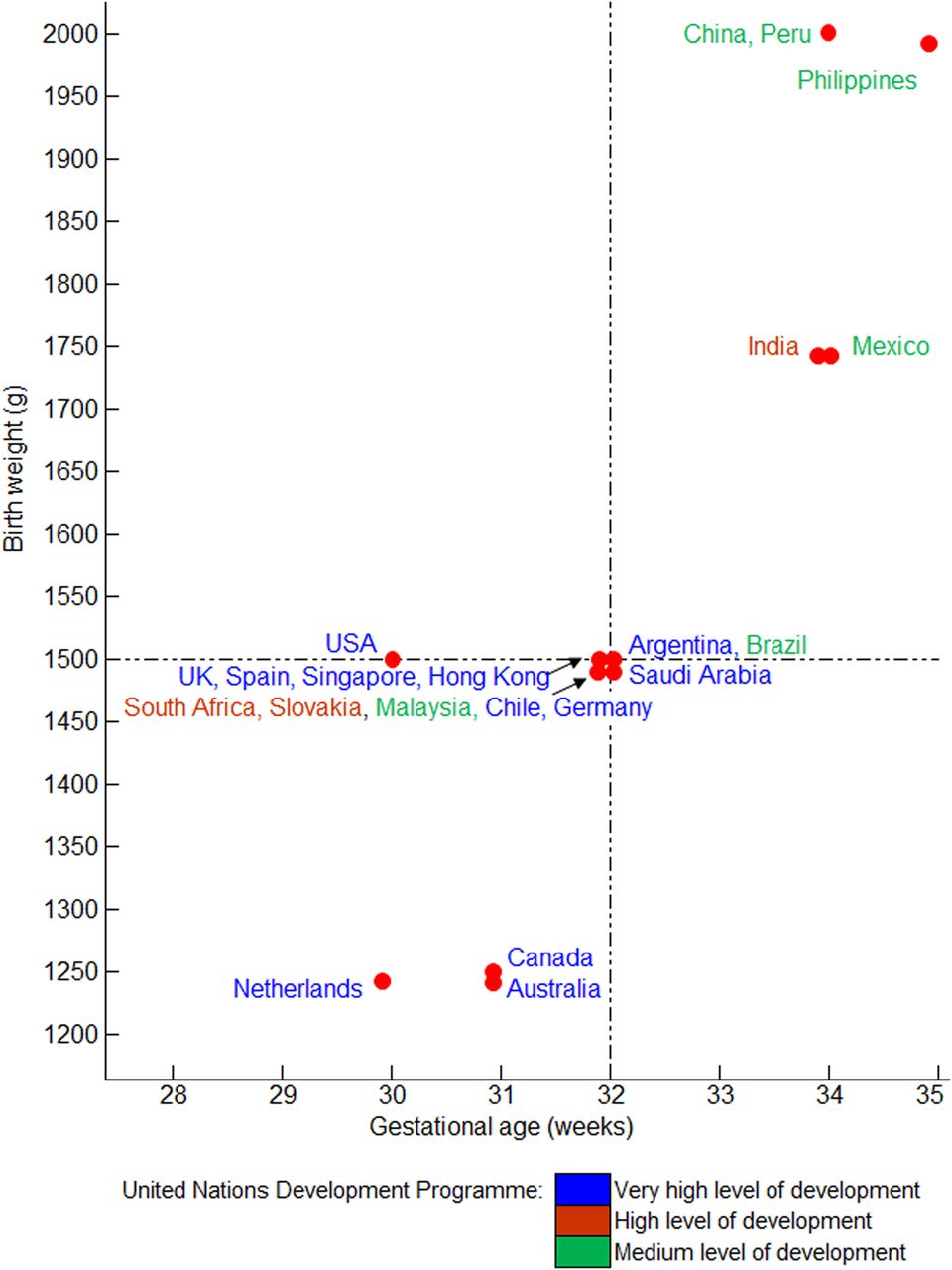
It has been recognised for almost two decades that sight-threatening ROP can affect more mature infants in settings where levels of neonatal care are suboptimal, and this is reflected in variation in the criteria for ROP screening in national guidelines (figure 1). All the guidelines represented in figure 1 were developed or have been revised since 2004 and were based on local evidence. All countries with very high levels of development, based on the United Nation's Human Development Index, have criteria that fall within a gestational age (GA) of ≤32 weeks or a birth weight (BW) of ≤1500 g, including Sweden, which uses only one criterion of GA of <31 weeks. Countries with lower development indices tend to use wider criteria, reflecting the population at risk.
{kind=link}
Gestational age and birthweight indications for screening for retinopathy of prematurity in different countries.
Countries that have not yet developed evidence-based criteria need to adopt wider BW and GA criteria than anticipated in the first instance, and data need be recorded from a large number of infants in a range of units in order derive guidelines that reflect the variation in care between neonatal units, as in the Oman study.2 Plotting BW against GA can assist in delineating safe criteria for screening.3 ,4 Indications for screening are likely to continue to vary as long as the population at risk of sight-threatening ROP varies, and so one size will not fit all. Indeed, in the Oman study 8% of infants requiring treatment would not have been screened if criteria from the USA had been applied.
As well as variation in eligibility criteria for screening, the timing of the first examination also varies between countries. Many highly developed countries use GA to guide the postnatal age at which the first examination should take place, which is possible in situations where GA can be accurately determined by early fetal ultrasound. However, in many countries attendance at antenatal care can be low, fetal ultrasound is not routinely available and many mothers of preterm infants are poorly educated or teenagers who do not know the date of their last menstrual period. In these settings, rates of intrauterine growth restriction can be also be high, making clinical assessment of GA unreliable. As a consequence, some countries have less complex recommendations for the timing of the first examination: in India, for example, the National Neonatology Forum guidelines (2010) advocate that the first examination be performed by 30 days of life in infants born with a GA of ≥28 weeks. Infants born at <28 weeks or with a BW of <1200 g should be screened earlier, by 2–3 weeks of age, to enable early identification of aggressive-posterior ROP. Complex guidelines regarding timing of the first examination can be difficult to implement when nursing levels are low and where a high proportion of nursing staff have received no formal training in neonatology, a frequent finding in many middle-income countries. Under these circumstances, a simple guideline, that is, at a fixed interval after birth, is more straightforward to implement.
In countries with lower levels of development, preterm infants can be discharged early, due to pressure on cots, and attendance at follow-up can be low, particularly if parents are poor and uneducated or live far from the neonatal unit. Indeed, relatively high rates of non-attendance for ROP screening after discharge have been reported in several countries. Screening before discharge, as a means of ensuring that all infants at risk have at least one examination, is a strategy that can be adopted. This is recommended in the Saudi Arabian guidelines for all infants with a GA of <32 weeks, and a recent study in India has demonstrated that a first examination of all eligible infants before discharge significantly increased compliance with screening.5 Given the variation in socioeconomic status of mothers and in health services for preterm infants, pragmatic decisions concerning the timing of the first examination are also likely to continue to vary.
As well as variation in the indications for screening and the timing of the first examination, there is also increasing variability in who performs the screening and the approaches they use. The established practice is for ophthalmologists to examine infants in the neonatal unit on a regular weekly or biweekly basis, using indirect ophthalmoscopy or, where resources allow, digital imaging using a wide-field camera (RetCam). This entails examining a large number of infants in order to identify the relatively few who develop ROP needing treatment. This is a challenge in all locations, but the main reasons vary. In some countries, there is a lack of ophthalmologists overall and a severe shortage of ophthalmologists skilled in indirect ophthalmoscopy, paediatric ophthalmology or medical retina. In other countries, there are an adequate number of skilled ophthalmologists, but as screening is often not included in salaried time, only the most committed are willing to screen. Ophthalmologists may also be reluctant to screen because of medico-legal concerns or because of opportunity costs. As a consequence, an increasing number of centres use trained nurses to take the retinal images, with interpretation by an ophthalmologist with expertise in ROP. In Karnataka state in India, another approach has been adopted in which trained technicians take the wide-field images and interpret them at the cotside, once they have reached adequate levels of competency.4 Images of infants where the technician considers treatment to be indicated are reviewed remotely in real time by an ROP expert. This innovative approach has resulted in massive scale-up of ROP screening as five teams can visit 90 neonatal units every week. Over 8 years, >75 000 imaging sessions have been undertaken on >23 000 preterm infants and >1500 infants have been treated for type 1 ROP (where urgent treatment is indicated).6 With greater access to the internet, remote interpretation of images by ophthalmologists or trained technicians is likely to increase and software for automated image analysis is also on the horizon as are cloud-sourcing and machine learning approaches. Whichever approach is used to interpret images, high levels of validity are essential not only to accurately identify all infants with the constellation of clinical signs that indicate the need for urgent treatment but also for the other important management decisions, that is, no further screening examinations are required, or further examinations are required, and when. New, lower-cost wide-field digital cameras are also on the horizon, which offer the potential for staff in the neonatal unit to capture the retinal images, with interpretation using one of the approaches outlined above.7 There is, therefore, potential for even greater variability in screening approaches in the foreseeable future.
There are several other areas of active research in relation to screening for ROP, which may lead to greater variability in practices. For example, if valid biomarkers of subsequent risk of sight threatening ROP were to become available, such as early serum levels of growth factors, this would allow countries with adequate resources to use these biomarkers to refine their indications for screening. Early weight gain is a low-cost marker that is feasible to implement, but although predictive in some populations this is not universally the case.8
ROP is becoming a global public health problem. Given the wide variation in health systems and health financing between countries as well as variation in the socioeconomic status of families of preterm infants, screening for ROP will need to be responsive to local settings. It is also imperative that screening for ROP only be undertaken where there are resources for prompt, high-quality treatment that is accessible and affordable. New and emerging technologies will bring new opportunities as well as challenges in screening for ROP. One size does not and will not fit all—nor should it.
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; internally peer reviewed.