Article Text

Abstract
Aims: To report the histopathology of two specimens of polypoidal choroidal vasculopathy (PCV) obtained from two eyes of Japanese patients.
Methods: Specimens were obtained under direct visualisation during macular translocation surgery with 360 degree retinotomy. The clinical findings were correlated with the light microscopic findings of the two specimens.
Results: One specimen from a 77 year old man was the central portion of the lesion that lay under the sensory retina on the retinal pigment epithelium (RPE). The specimen was made up mainly of fibrous tissue with small, thin walled vessels. Indocyanine green angiography after surgery revealed that active leaking polypoidal element remained under the RPE. Another specimen obtained from a 62 year old man was made up of a fibrovascular membrane situated within Bruch's membrane. The part of this specimen inferior to the foveal region included a collection of dilated, thin walled blood vessels without pericytes, surrounded by macrophages that stained positive for CD68. The dilated vessels appeared to be correlated with the orange coloured polyps observed by ophthalmoscopy, the polypoidal structure seen in indocyanine green angiograms, and the pyramidal elevation with intermediate reflectivity by optical coherence tomography.
Conclusion: Polypoidal structures are located within Bruch's space. They are composed of clusters of dilated, thin walled blood vessels surrounded by macrophages and fibrin material. The positive immunohistochemical staining for vascular endothelial growth factor in the RPE and the vascular endothelial cells suggests that this fibrovascular complex is a subretinal choroidal neovascularisation.
- polypoidal choroidal vasculopathy
- macular translocation
- histopathology
Statistics from Altmetric.com
Polypoidal choroidal vasculopathy (PCV) was first described by Yannuzzi1 in 1982, and he and his colleagues published2 their observations on this peculiar vascular abnormality in the choroid as a new clinical entity. Stern et al3 and Perkovich et al4 described a similar condition and called it a “multiple recurrent serosanguineous retinal pigment epithelial detachment” that was commonly found in black women. Kleiner et al reported the same condition but called it a “posterior uveal bleeding syndrome.”5
In these earlier articles, the peripapillary location of the polypoidal choroidal vascular abnormality was emphasised. In 1998, Moorthy et al described seven patients with polypoidal lesions stemming from the macular choroidal circulation that could be confused with age related macular degeneration if indocyanine green angiography was not performed. 6
PCV is reported to be more common in black and Asian people.7 In a series of 35 eyes of Japanese patients, the lesions were mostly (94%) in the macula.8 The final visual acuity of Japanese patients with PCVs after a follow up of 20 months without treatment was reported to be linearly related to the initial visual acuity.8 The polypoidal lesion in white people was also reported to be predominantly in the macula,9 and the location of the lesions and the associated fundus lesions were reported to be very similar to those of exudative age related macular degeneration. Some patients have leakage from secondary classic or occult choroidal neovascularisation.6–11 In the presence of coexisting subfoveal choroidal neovascularisation with exudation, the visual prognosis should be as poor as that of exudative age related macular degeneration or even poorer because of the tendency to be associated with large subretinal haemorrhage and/or vitreous haemorrhage.11 However, the clinical feature is reported to have a large clinical spectrum.11,12
One of the reasons that the pathogenesis of this disease and its essential difference from age related macular degeneration is not well established is because only four specimens of PCV have been studied histopathologically.13–16 Of these four eyes, two eyes were enucleated because of rubeosis iridis and acute angle block glaucoma because of massive subretinal haemorrhage.13,14 Thus, both of these eyes may have had secondary histopathological changes. The other two specimens were surgically removed: one was removed through an intentional retinal break and included only the fibrous tissue between the retina and the retinal pigment epithelium (RPE) without the polypoidal vascular complex; and the other and most recent report, the entire submacular specimen was removed during vitrectomy possibly in combination with macular rotation.15,16 Although the fluorescein and indocyanine green angiographic findings before surgery were presented, the surgical procedures, the appearance during surgery, surgical results, and angiographic findings after surgery were not presented or correlated with the histological findings.
The identification of macular PCV and associated choroidal neovascularisation is important because the visual prognosis and management may be different from both the peripapillary type of PCV and age related macular degeneration with which it can be confused.
To understand more about the nature of this disease, we histopathologically examined two specimens of PCV obtained under direct visualisation during macular translocation surgery. The preoperative and postoperative fluorescein and indocyanine green angiograms, optical coherence tomographic images, and the final visual results were correlated with the histopathological findings.
CASE REPORTS
Case 1
A 77 year old man was referred to us on 10 April 2000 because of a progressive loss of vision in the right eye during the previous 7 months. His visual acuity was 20/400 in the right eye and 20/20 in the left. The ophthalmological findings in his left eye were unremarkable. The right eye had undergone phacoemulsification with intraocular lens implantation 2 months before he visited us. He had a history of hypertension that was controlled by daily medication.
Ophthalmoscopy of the right eye revealed a large retinal elevation in the macula over a subfoveal neovascular membrane with macular oedema and intraretinal haemorrhages. Optical coherence tomography (OCT 2000, software version A 4.01; Humphrey Instruments, San Leandro, CA, USA) showed that the elevation of the sensory retina was caused by a highly reflective mass with moderate internal reflection above a linear, horizontal highly reflective band corresponding to the RPE (Fig 1A).

Case 1. (A) Preoperative fundus photograph and vertical optical coherence tomographic scan (OCT) of the right eye. The yellow arrow points to the location of the cross sectional scan and possible pathological section. OCT shows an elevation of the sensory retina by a relatively highly reflective mass. The mass shows moderate internal reflection above the horizontal, linear, highly reflective band corresponding to the retinal pigment epithelium. (B) Fluorescein angiogram revealing a granular hyperfluorescence around the macula with a small amount of leakage around the fovea. (C) Indocyanine green angiogram demonstrating a branching vascular network superior to the fovea and polyp-like dilatations at the terminals of the branches nasosuperior to the fovea. (D) Postoperative fundus photograph and OCT at the newly located macula (white vertical bar = 250 μm). (E) Fluorescein angiogram 3 months after surgery showing the site of fluorescein leakage from the remaining polypoidal lesion at the previous macula. Also, cystoid macular oedema can be seen at the newly located macula. (F) Indocyanine green angiogram revealing polyp-like lesions with an associated network at the superior vascular arcade at the original site of the macula.
Fluorescein angiography revealed granular hyperfluorescence around the macula with a small amount of leakage around the fovea (Fig 1B). Indocyanine green angiography revealed a branching vascular network superior to the fovea with polyp-like dilatations at the terminals of the branches nasosuperior to the fovea (Fig 1C).
A diagnosis of PCV with a subfoveal neovascular membrane between the sensory retina and the RPE was made. An extensive discussion was held with the patient. The discussion included an explanation of the finding that the final visual acuity of Japanese patients with PCVs was reported to be linearly related to the initial visual acuity,8 and that the treatment options included only observation or removal of subfoveal CNV with or without macular translocation. Because of the CNV, the visual prognosis was considered to be as poor as age related macular degeneration, and after obtaining the patient's consent, we treated the eye with removal of the subfoveal membrane combined with macular translocation.
Surgery was performed on 12 May 2000. Our technique was a modification of the 360 degree retinotomy method of Machemer.17 A complete removal of the vitreous by pars plana vitrectomy, and the creation of four separate dome-shaped retinal detachments by the subretinal infusion of balanced salt solution (BSS-plus, Alcon, Fort Worth, TX, USA) was performed. Fluid-air exchange was then carried out that led to the coalescence of the four detachments followed by 360 degree retinotomy at the ora serrata with an automated scissors. After the retina was totally detached and inverted, the subretinal neovascular membrane was removed with forceps under direct visualisation. The irrigation pressure was set to 80 mm Hg for 2 minutes to prevent bleeding. No retinal pigment epithelial tear was found. This was followed by the injection of heavy perfluorocarbon liquid, rotation of the whole retina around the axis of optic disc with additional injection of perfluorocarbon liquid during the rotation, endophotocoagulation and the silicone oil-perfluorocarbon liquid exchange. Six weeks after this surgery the silicone oil was removed.
The final angle of retinal rotation was 40 degrees. Because the patient did not complain of diplopia after surgery, muscle surgery was not performed. OCT showed an almost normal macular configuration with a foveal depression (Fig 1D). Fluorescein and indocyanine green angiography showed residual larger and leaking polypoidal elements which were located under the RPE at the previous macula (Fig 1E, F). At the site of newly located macula, staining with fluorescein was noted (Fig 1E). Laser photocoagulation of the polypoidal lesions and a part of the associated network was performed soon after surgery that resulted in reducing the hyperfluorescence. However, polypoidal lesions recurred at the temporal side of the remaining vascular network at the previous macular site 8 months after surgery. These lesions were followed without treatment. The patient's best corrected visual acuity 6 months after surgery was 20/30 in the right eye.
Case 2
A 62 year old man was referred to us on 12 August 1998 for progressive loss of vision in both eyes. His visual acuity was 20/200 in the right eye and 20/60 in the left. He had no history of hypertension or other systemic diseases.
Ophthalmoscopically, there was a macular subretinal fibrovascular scar in his right eye and a haemorrhagic retinal pigment epithelial detachment with a small subretinal haemorrhage in his left eye. After 2 weeks, a large subfoveal haemorrhage developed in his left eye and visual acuity dropped to 20/200. Pneumatic displacement of subretinal haemorrhage was performed followed by radiation therapy for the subretinal neovascular membrane. After 6 months, his visual acuity recovered to 20/40, but then deteriorated after 6 months to 20/1000. At that time, ophthalmoscopy revealed macular oedema with lipid exudates, several orange-red lesions under the sensory retina and thin subretinal haemorrhages. OCT showed an oedematous elevation of the sensory retina. Above the highly reflective line corresponding to the RPE, a small dome-shaped elevation with another highly reflective line was observed. The two pyramidal elevations of the RPE with moderate internal reflection at the lower and upper end of the vertical section corresponded to the orange-red lesion seen in the macula by ophthalmoscopy (Fig 2A).

Case 2. (A) Preoperative fundus photograph and vertical optical coherence tomography scan (OCT) of the left eye. Macular oedema with lipid exudate, several orange-red lesions, and thin subretinal haemorrhage can be seen. OCT shows an oedematous elevation of the sensory retina. A small dome-shaped elevation showing another highly reflective line can be seen above the high reflective line corresponding to the retinal pigment epithelium. Two pyramidal elevations of the retinal pigment epithelium with moderate internal reflection at the upper and lower end of the vertical section corresponding to the orange-red lesions seen by ophthalmoscopy can be seen. (B) Fluorescein angiogram revealing granular hyperfluorescence around the macula with relative hypofluorescence at the centre. (C) Indocyanine green angiogram revealing subfoveal choroidal neovascularisation and polyp-like dilatations at the terminals of the branches around the fovea. The associated vascular networks cannot be seen. (D) Postoperative fundus photograph and OCT by vertical scan (white vertical bar = 250 μm.) (E) Fluorescein angiogram showing a large area of hyperfluorescence and extensive defect of the retinal pigment epithelium at the previous macula. An RPE rip can also be seen superior to the disc (arrow). (F) Indocyanine green angiogram showing atrophy of the choriocapillaris at the previous site of the macula without polypoidal lesions or vascular network.
Fluorescein angiography revealed granular hyperfluorescence around the macula with relative hypofluorescence at the centre that suggested a subfoveal neovascular membrane with scattered vascular components. Indocyanine green angiography revealed neovascularisation under the fovea and polyp-like dilatations at the terminals of the branches around the fovea. The associated vascular networks could not be observed because of the blockage of fluorescein by the serous fluid (Fig 2B). Late phase indocyanine green angiography also revealed hypofluorescence at the fovea that suggested a subfoveal fibrous membrane with poor vascularity. (Fig 2C).
A diagnosis of PCV with a subfoveal neovascular membrane between the sensory retina and the RPE was made. After extensive discussion with the patient and the presentation of the results on previous Japanese patients with PCV, and the treatment options including only observation, removal of subretinal membrane with or without macular translocation, he agreed to be treated by a removal of subfoveal membrane combined with macular translocation, because in the presence of subfoveal CNV, the visual prognosis was considered to be as poor as age related macular degeneration or even poorer because of recurrent subretinal haemorrhages.
Surgery was performed on 7 November 2000 with a technique that was very similar to that of case 1. Before the vitrectomy, pars plana lensectomy with preservation of the anterior capsule was performed. After the retina was totally detached, an attempt was initially made to remove the thin subretinal neovascular membrane on the RPE. Because the subretinal membranous tissue was connected to the subretinal pigment epithelial vascular complex, the whole subretinal and sub-RPE vascular complex including RPE was removed, resulting in the large defect of the RPE. The RPE defect is a concomitant complication of this surgery. Twelve weeks after this surgery the silicone oil was removed.
The angle of retinal rotation was 45 degrees, and muscle surgery was delayed for a later time. His best corrected visual acuity 3 months after surgery was 20/300 because of the atrophy of the RPE beneath the new fovea that had been located next to the vascular complex. OCT showed almost normal macular configuration with a foveal depression; however, the retina was thinner than normal (Fig 2D).
Fluorescein angiography showed a large area of hyperfluorescence due to the extensive RPE defect at the previous macula. An RPE rip was also noted superior to the disc (Fig 2E). Indocyanine green angiography revealed atrophy of the choriocapillaris at the previous macula site without polypoidal lesions or vascular network (Fig 2F).
Histopathology
The resected tissue was fixed in 10% formalin and embedded in paraffin. Serial 4 μm sections were cut and stained with haematoxylin and eosin (except for unstained slides for special staining). All of the stained slides were evaluated histologically by light microscopy (Eclipse E600, Nikon, Tokyo, Japan).
Immunohistochemical studies were performed on paraffin sections using avidin-biotin complex method on an automated immunostainer (HX System, Ventana, Tucson, AZ, USA) as described previously.18 The tissue were evaluated with the following antibodies: CD34 (Qubend 10, 1:50, Dako, Kyoto, Japan), α-smooth muscle actin (1A4, 1:50, DAKO, Kyoto, Japan), vimentin (V9, 1:50, Dako), CD68 (KP-1, 1:50), and vascular endothelial growth factor (VEGF, C-1, 1:100, Santa Cruz, Santa Cruz, CA, USA). Histochemical stains such as periodic acid Schiff (PAS) stain for basal membrane, phosphotungstic acid haematoxylin (PTAH) stain for fibrin, and elastica van Gieson stain for elastic fibre were also performed.
In case 1, fibrovascular tissue was seen to be located between the sensory retina and the RPE as had been observed with the operating microscope. Indocyanine green angiography after surgery demonstrated that the tissue removed was the subretinal part of the neovascular lesion, and the large leaky polypoidal lesion and associated vascular network under the RPE remained at the previous macula. Most of this specimen contained fibrous tissue with some small, thin walled vessels (Fig 3).

Case 1, histopathology. (A) Subretinal fibrovascular tissue (haematoxylin and eosin, original magnification ×10). (B) A high power photomicrograph of the region outlined by the yellow box in the upper figure. The specimen is made up of mainly fibrous tissue with some small thin walled vessels (haematoxylin and eosin, original magnification ×100).
The histopathology of the removed specimen resembled that of a subretinal neovascular membrane in age related macular degeneration, and was characterised by fibrovascular membranes with endothelium lined vascular channels similar to granulation tissue.19
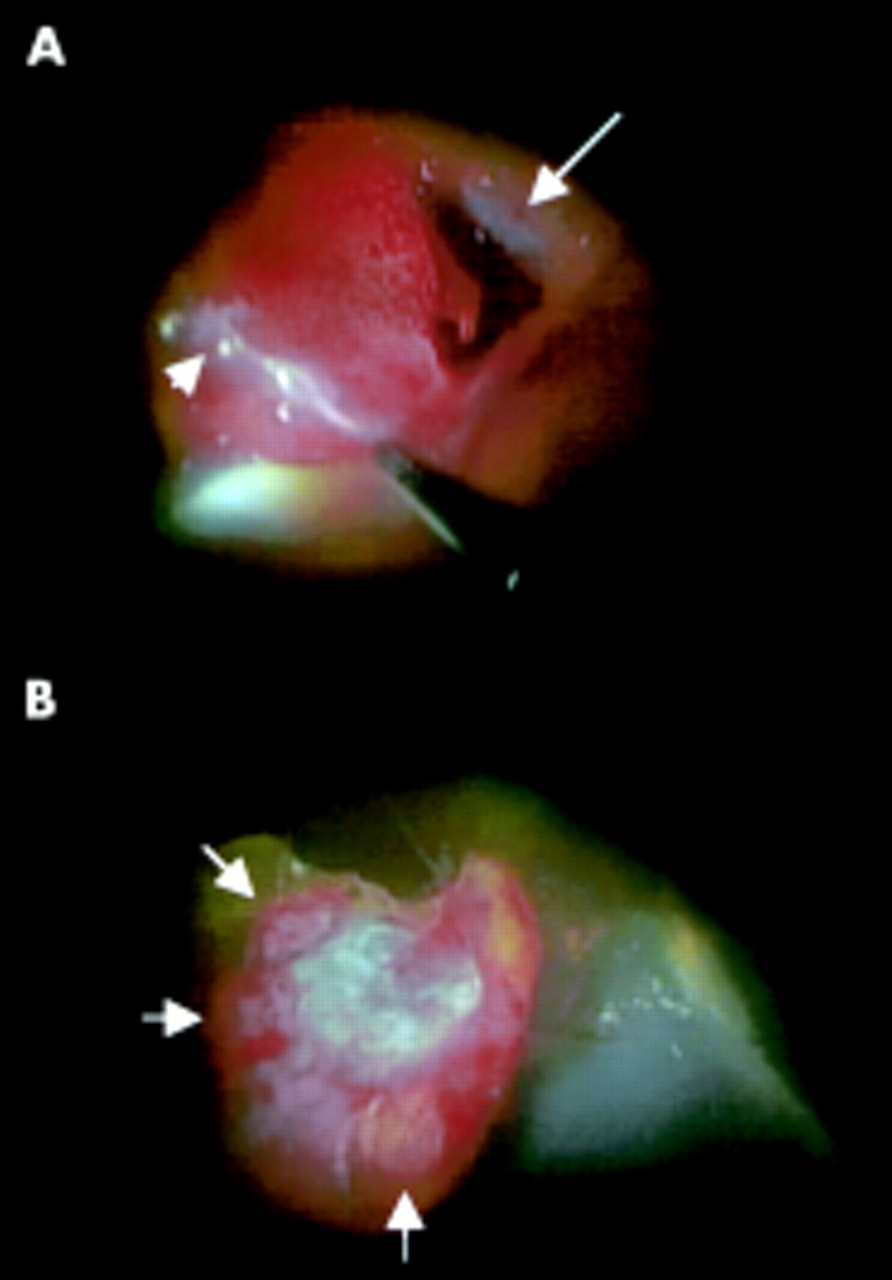
The specimen from case 2 showed a similar fibrovascular tissue; however, it was located under the RPE and within Bruch's membrane. It had been removed with the RPE after peeling the thin fibrous membrane above the RPE under direct visualisation through the operating microscope. The observation of the fibrovascular tissue with the RPE under the operating microscope revealed that this fibrous tissue contained dilated vessels that were seen from the choroidal side of the tissue (Fig 4).

Case 2. Photographs from videophotography taken during surgery. (A) After peeling the thin fibrous membrane on the retinal pigment epithelium (short arrow), the subretinal pigment epithelial fibrovascular complex was removed with the retinal pigment epithelium (RPE). Large arrow indicates RPE tear. (B) Photograph of the choroidal side of the resected tissue under the operating microscope. White fibrous tissue is surrounded by clusters of relatively large vessels (arrows).
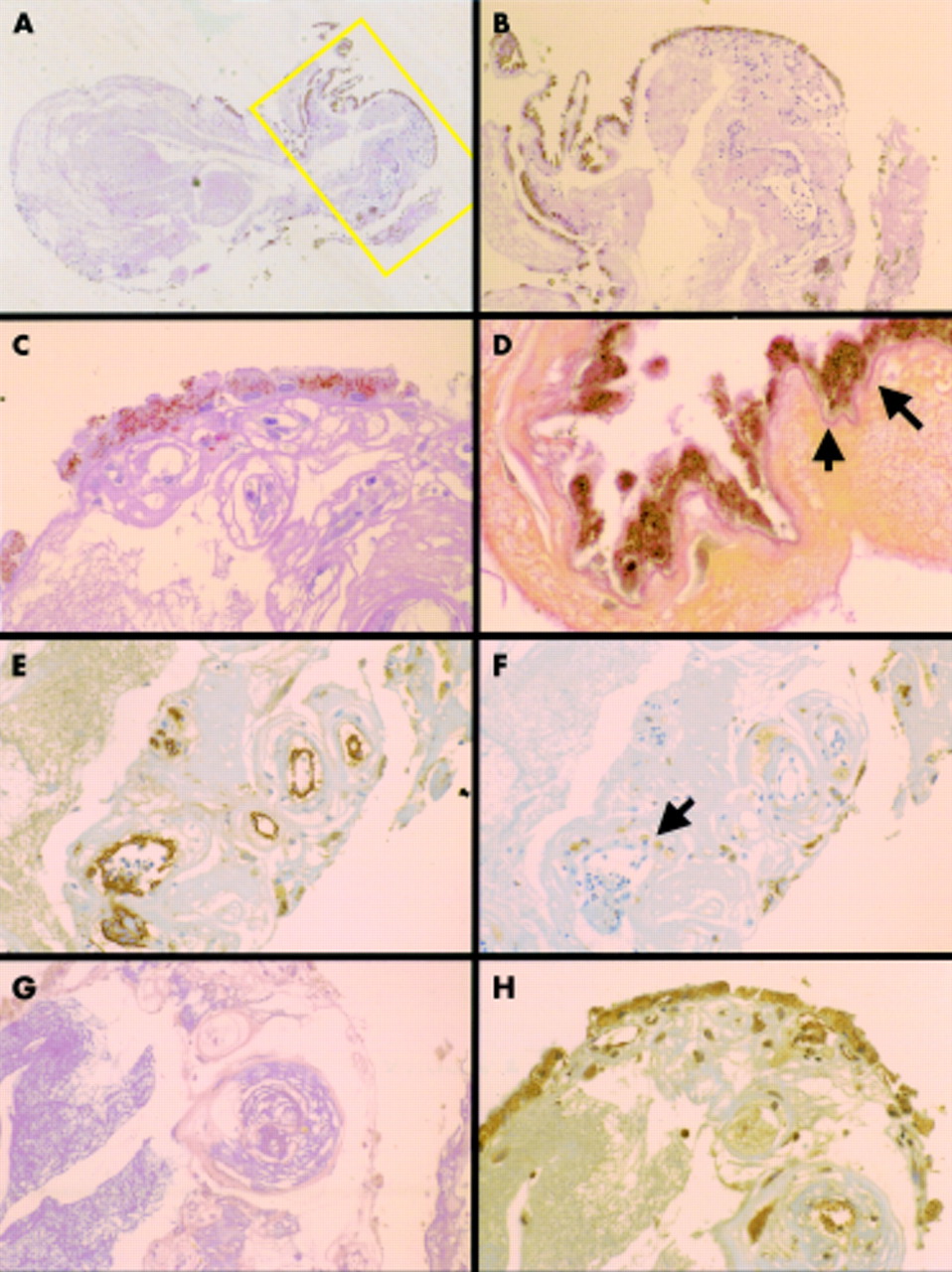
Histologically, the fibrovascular tissue was located under the basement of the RPE and the elastic fibre layer of Bruch's membrane, which was stained by the elastica van Gieson method. The fibrovascular tissue contained a number of dilated, thin walled vessels, and these vessels seemed to correspond to the polypoidal lesions seen ophthalmoscopically and by indocyanine green angiograms. We could not find the arteriole and venule at the fibrovascular ingrowth site from the choroid to the fibrovascular tissue in our histological sections. The abnormal vessels were lined by a thin endothelium stained by CD34 without pericytes. The immunohistochemical stain to α-smooth muscle actin for the smooth muscle of blood vessels was negative. Macrophages had infiltrated around the dilated vascular cavity and stained positively for CD68 by immunohistochemical staining. The vessels were surrounded by a massive leakage of fibrin material as demonstrated by the staining with PTAH stain for fibrin. The immunohistochemical stain to vimentin for mesenchymal tissue was positive in the RPE and endothelial cells. A positive staining for vascular endothelial growth factor in the RPE and vascular endothelial cells was demonstrated (Fig 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 2, histopathology. (A) Subretinal pigment epithelial fibrovascular tissue (haematoxylin and eosin, ×10). (B) A high power photomicrograph of the region outlined by the yellow box in (A). The fibrovascular tissue contains a collection of dilated, thin walled vessels that appear to correspond to the polypoidal lesions seen by ophthalmoscopy and indocyanine green angiography (haematoxylin and eosin, original magnification ×40). (C) Fibrovascular tissue can be seen under the basement membrane of the retinal pigment epithelium. (periodic acid Schiff, original magnification ×200). (D) The mass is seen under the elastic fibre layer of Bruch's membrane indicated by the arrows—that is, intra-Bruch's space (elastica van Gieson, original magnification ×400). Immunohistochemical and histochemical stains. (E) Abnormal vessels are lined by a thin endothelium without pericytes and are positive for CD34 (immunohistochemical stain for CD34, original magnification ×100). (F) Infiltration of macrophages around the large lumen vessels indicated by an arrow can be seen (immunohistochemical stain for the CD 68, original magnification ×100). (G) Massive leakage of fibrin material is seen in large area of specimen. Fibroblastic cells surrounded the fibrin materials around the vessels (phosphotungstic acid haematoxylin histochemical stain for fibrin, original magnification ×100). (H) Positive stain for antivascular endothelial growth factor in the retinal pigment epithelium and vascular endothelial cells (immunohistochemical stain for antivascular endothelial growth factor, original magnification ×100).
DISCUSSION
The histopathological examinations demonstrated that the polypoidal structures were located within Bruch's space and were composed of clusters of dilated, thin walled blood vessels surrounded by fibrin material. Ophthalmoscopically, both lesions were located in the macula. In a series of Japanese8 and white9 patients with PCV, the lesions were also found mostly in the macula, and some patients retained relatively stable visual acuity compared to patients with age related macular degeneration. In a study of 35 Japanese patients,8 31 patients had visual acuity of better than 20/200 at the final follow up; however, the final visual acuity was worse in one patient with visual acuity of 20/1000 and the three patients with 20/200 at the first visit. Considering vision for reading, 29% of the 35 eyes had a final visual acuity of 20/100 or worse because of recurrent subretinal haemorrhages, serous retinal detachments, and disciform scars.
The location of the lesions and the appearance of fundus lesions in eyes with PCV in the Japanese were reported to be very similar to that in eyes with exudative age related macular degeneration. There appears to be a demographic difference of the PCV described in black patients and those in Japanese and white populations; PCV in black patients showed characteristic polypoidal lesions originating from the peripapillary choroidal circulation, while the PCV in both Japanese and white patients originated mainly from the macular choroidal circulation. The plaques visualised by indocyanine green angiography in 26 of 45 eyes of white patients9 were an indirect demonstration of the association of submacular neovascular membranes to this disease. From these results, PCV can be considered to be associated with exudative age related macular degeneration, although it should be generally treated as a distinct clinical entity.
MacCumber et al13 were the first to report on the pathological findings in an eye with the clinical appearance of “multiple recurrent serosanguineous pigment epithelial detachment syndrome.” This eye exhibited a thick fibrovascular membrane extending to the mid-periphery within Bruch's membrane with many sites of vascular ingrowth from the choroid into Bruch's membrane. The fibrous tissue and choroid contained many inflammatory cells. The difficulty of interpreting the findings in this eye is that the changes may have been secondary to the longstanding multiple haemorrhages, phthisis, hypertension, and diabetes mellitus. Indocyanine green angiography was not performed before the enucleation and, later, the fellow eyes failed to demonstrate polyps.
In another enucleated eye with angle blockage glaucoma by a massive subretinal haemorrhage,14 the fibrovascular membrane was also located within Bruch's membrane without a subretinal component. The presence of bilateral polypoidal structures had been demonstrated previously but the authors did not find aneurysmal vessels in the histological specimen.
Shiraga et al15 reported on the histological findings of a surgically excised membrane, which had developed after removal of a submacular haemorrhage. The tissue showed only subretinal fibrovascular tissue under the sensory retina and above the RPE without a polypoidal vascular complex, which was considered to represent the subretinal part of the neovascular membrane similar to our specimen in case 1.
The most recent report described the entire submacular tissue specimen.16 An intra-Bruch's fibrovascular membrane was seen with saccular, thin walled aneurysmal vessels that appeared to be of venular rather than arteriolar origin. The characteristic aneurysmal vessels were located immediately under diffuse drusens. This specimen was probably obtained during vitrectomy possibly in combination with macular rotation. However, the acquisition and reason for the excision were not described clearly. Additionally, the authors did not mention whether their specimen was correlated with the fundus findings and observations during surgery. The surgical results and angiography after surgery were also not described.
Thus, the histopathological findings in PCV and their correlation with clinical findings are limited. Our histological specimen in case 2 was removed under direct visualisation with the operating microscope after the retina was detached and inverted. The observation of the removed fibrovascular tissue with the RPE under the operating microscope revealed that this fibrous tissue contained relatively large vessels when examined from the choroidal surface.
Histologically, the fibrovascular tissue was located under the RPE and its basement membrane stained diffusely with PAS, and under the elastica of Bruch's membrane stained by the elastica van Gieson method—that is, intra-Bruch's space. The fibrovascular tissue contained a collection of dilated, thin walled vessels, which appeared in serial sections to be connected to each other. This collection of vessels appeared to correspond to the polypoidal lesion demonstrated by ophthalmoscopy and by indocyanine green angiography. However, we were not able to find the arteriole and venule entering the fibrovascular ingrowth from the choroid. The abnormal vessels were lined by a thin endothelium without pericytes and smooth muscles, and there was massive leakage of fibrin material around the vessels. A number of macrophages were found around the dilated vascular cavity as demonstrated by the immunohistochemical stain with CD68, although it was unclear whether these macrophages were related to the inflammation. They may have infiltrated the lesion to perform a phagocytic role for the intravascular materials that leaked through the loose vascular walls.
The positive immunohistochemical stain for vascular endothelial growth factor in the RPE and vascular endothelial cells suggested that vascular endothelial growth factors may have been one of the stimulators of vascular membrane neogenesis in this disease. Thus, we conclude that the vascular complex including fibrovascular membrane and polypoidal structure was a choroidal neovascularisation.
In case 1, a similar fibrovascular tissue was removed, but it was located between the sensory retina and the RPE as was observed by direct visualisation under the operating microscope. The indocyanine green angiography after surgery revealed that the tissue removed was the subretinal part of the neovascular lesion, and the polypoidal lesion and associated vascular network under the RPE remained as it was at the previous macula. The histopathology of the removed specimen showed that it was from the central portion of the lesion rather than the larger and leaking polypoidal elements. The specimen resembled that of classic CNV in age related macular degeneration, while the remaining active leaky polypoidal lesion might have had the more typical histological appearance as in case 2. Thus, because of the location of the polypoidal elements, indocyanine green angiography should be performed to make a correct diagnosis and to differentiate this disease from classic CNV in AMD and central serous chorioretinopathy.12
Some patients with PCV have been shown to have chronic recurrent serosanguineous detachments of the RPE and neurosensory retina resulting in the atrophy of the central retina with severe vision loss. Other patients have experienced vitreous haemorrhage or secondary CNV with disciform scarring and profound loss of central vision. The vascular lesions of PCV are characterised by their variability in size, location and clinical course, and progressive enlargement of the vascular elements has been documented in the series of Yannuzzi et al.11
In our case 2, the whole polypoidal vascular complex was successfully removed from the macula during macular translocation surgery which stabilised the visual acuity, and the poor visual outcome resulted from the long history of exudative maculopathy with recurrent subretinal haemorrhage.
One of the treatment options for PCV is photocoagulation of the polypoidal vascular lesions.2 Resolution of the serosanguineous detachments associated with the peripapillary or paramacular lesions would be expected, but the use of photocoagulation for macular lesions should be guarded. Surgical drainage of a subretinal haemorrhage has also been reported to be beneficial for eyes with PCV. However one eye, that had a subretinal haemorrhage removed, developed a neovascular membrane soon after surgery which was also removed surgically. The final visual acuity in this eye was 20/500.15
For age related macular degeneration, macular translocation surgery is one choice to rescue useful vision. Considering that PCV may possibly be a peculiar variant of exudative age related macular degeneration,6–9,16 photodynamic therapy should also be considered for the preservation of some useful vision.
Although large leaking elements were present at the macula in case 1 and large wheel-like polypoidal structures in case 2, the quiescent vascular component represented by the fibrous component in these two eyes might suggest the possibility of regression of active membranes.
In conclusion, we have correlated the clinical findings of eyes with PCV to the histopathology of the specimens which were removed under direct visualisation during macular translocation surgery. However, the exact clinicopathological correlation of the area was not possible because of a lack of the orientation of the specimens. One specimen was from the subretinal portion of the neovascular membrane without the polypoidal elements. The other specimen was an intra-Bruch's polypoidal vascular complex with the RPE. The polypoidal vascular lesion contained dilated, thin walled vessels without pericytes which corresponded with the orange coloured polyp. These vessels were surrounded by macrophages and amorphous proteinaceous material stained for fibrin. The location of the fibrovascular membrane with dilated vessels and the positive immunohistochemical stain to antivascular endothelial growth factor in the RPE and vascular endothelial cells suggested that the vascular components of this polypoidal vascular complex were not dilated choroidal vessels but a subretinal neovascularisation.
Acknowledgments
This study was supported by grant in aid No 11470363 and No 12470361 from the Ministry of Education, Science, Sports and Culture, Japan.