Article Text

Abstract
Aim To investigate the retinal nerve fibre layer (RNFL) with optical coherent tomography (OCT) in prematurely-born children.
Methods 62 children born with a gestational age of ≤32 weeks, and a control group of 54 children born at term with normal birth weight (BW) were included in the study. 28 of the preterm children had retinopathy of prematurity (ROP) in the neonatal period; eight of them had severe ROP (stages 3–4). RNFL thickness was measured with Stratus OCT 3. Mean age at examination was 8.6 years in the preterm children and 10.1 years in the control group.
Results There was a significant difference between the children born preterm and those born at term, regarding RNFL thickness in the superior (right eye (RE), p=0.043; left eye (LE), p=0.048) and the nasal quadrants (RE, p=0.006; LE, p<0.001), as well as average RNFL thickness (RE, p=0.016; LE, p=0.029). This difference was caused by the thinner RNFL in children with previous severe ROP (stages 3 and 4). Within the preterm group, the average RNFL thickness increased with larger BW (RE, p=0.050; LE, p=0.028), but there was no correlation with gestational age at birth.
Conclusion The RNFL was reduced in prematurely-born children with severe ROP when compared to children born at term. It is hypothesised that severe retinopathy as well as ablation of the retina with laser treatment or cryotherapy may affect the axons of the ganglion cells and thus reduce RNFL thickness. Prematurely-born children with low BW had a thinner RNFL, suggesting a negative effect of low birth weight on neural development.
- Prematurely-born children
- retinal nerve fibre layer thickness
- optical coherent tomography
- birth weight
- retinopathy of prematurity
- electrophysiology
- imaging
- genetics
- retina
- vision
- low vision aid
- epidemiology
- child health (paediatrics)
Statistics from Altmetric.com
- Prematurely-born children
- retinal nerve fibre layer thickness
- optical coherent tomography
- birth weight
- retinopathy of prematurity
- electrophysiology
- imaging
- genetics
- retina
- vision
- low vision aid
- epidemiology
- child health (paediatrics)
Perinatal and neonatal care in Western countries has improved dramatically in recent decades, with survival of children born as early as in the 22nd gestational week.1 Preterm birth may affect the child in many different ways,2 and the eye and visual function are no exception. Major complications like brain lesions and sequelae of retinopathy of prematurity (ROP), may lead to severe visual impairment.3 Several studies have shown that children born prematurely have subnormal visual acuity, a higher prevalence of refractive errors and strabismus, as well as reduced stereopsis, contrast sensitivity and visual fields.4–9 The cause of subnormal vision is not clearly understood. We have recently shown that the central macula measured with optical coherent tomography (OCT) is thicker in prematurely-born children than in children born at term, suggesting a disturbance in the retinal maturation caused by the preterm birth.10 Previous large cohort studies have shown that retinal nerve fibre layer (RNFL) thickness is affected by low birth weight, which could indicate that the ganglion cells are also affected by birth parameters.11 ,12
The aim of the present study was to measure RNFL thickness with OCT in children born prematurely and make comparisons with children born at term. A second aim was to determine whether ROP, neurological deficits or prematurity per se had any influence on RNFL thickness in the preterm group.
Materials and methods
Sixty-eight children born with a gestational age (GA) of 32 weeks or less at Uppsala University Hospital were included in the study. All of them had undergone routine screening for ROP, starting in the fifth postnatal week and continuing until the retina was fully vascularised or, in the case of ROP, the ROP was fully resolved. The stages of ROP were divided into mild ROP (stages 1–2) and severe ROP (stages 3–4). No child had ROP stage 5. The severe ROP group also included children who received laser treatment or cryotherapy for ROP. The criterion for treatment at that time was ROP stage 3 in at least four contiguous clock hours, with or without ‘plus’ disease.
Hospital records were used to locate the prematurely born children and their caregivers, who were invited by letter to participate in the study.
The control group, comprising 55 children born in Uppsala County, Sweden, was randomly selected from the birth register of the Swedish National Board of Health and Social Welfare. These children were born at term (GA ≥37 weeks) and had normal birth weights (BW ≥2500 g).13
Information regarding neurological complications, defined as intraventricular haemorrhage (IVH), cerebral palsy (CP), periventricular leucomalacia (PVL) and epilepsy, was obtained from the parents and from medical records. The best corrected visual acuity (VA) was assessed for each eye with linear logMAR charts. Cycloplegic retinoscopy and ophthalmoscopy were done 45 min after dilating the pupils with eye drops containing phenylephrine 1.5% and cyclopentholate 0.85%.
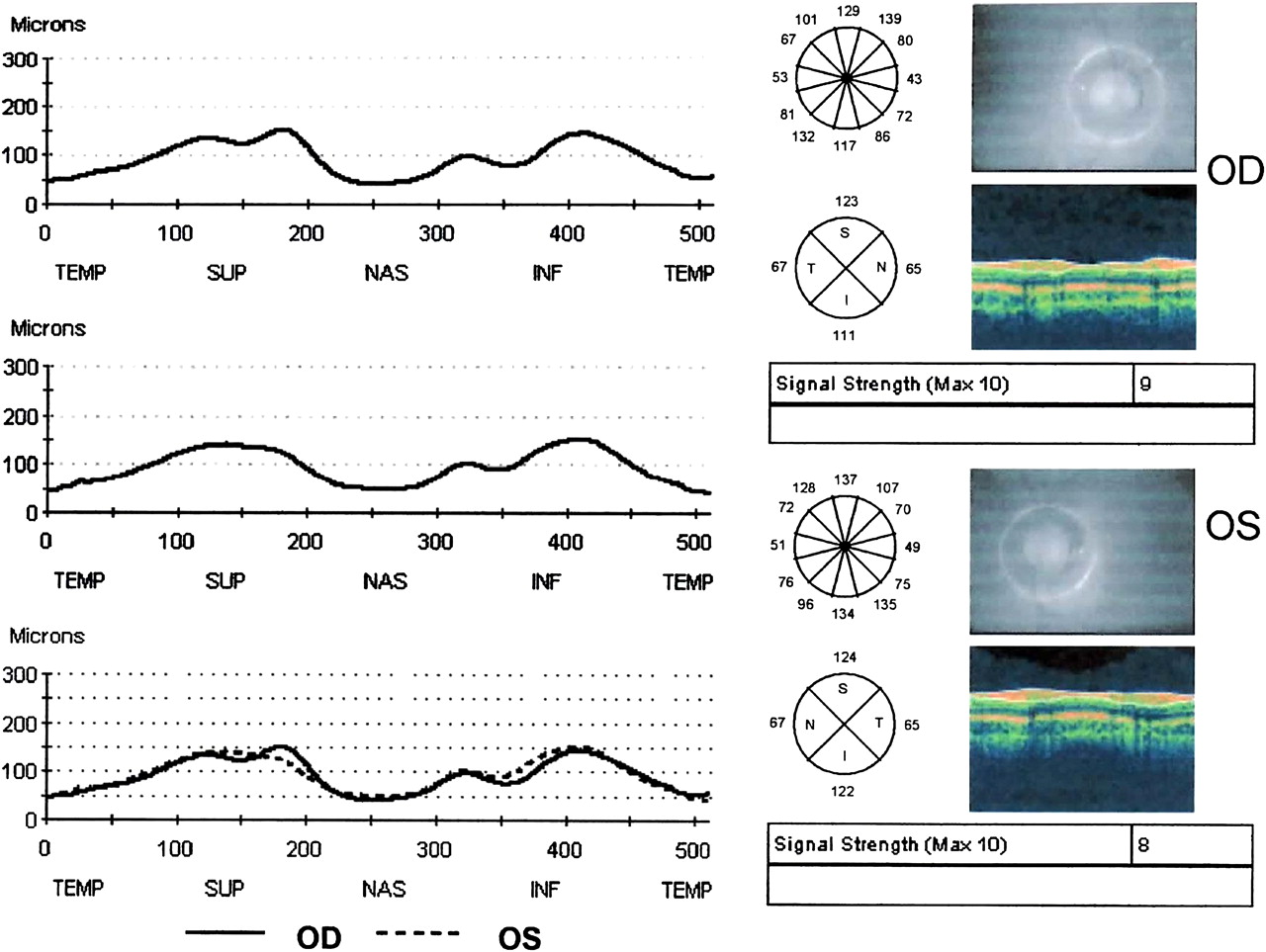
OCT uses low coherent light (near infrared light with a wavelength of 840 nm) to create a tomographic image of the retina. From this image it is possible to measure the thickness of the whole retina as well as the RNFL. Stratus OCT 3 (Version 4.0.1; Carl Zeiss Meditec, Dublin, California, USA) was used in this study. The peripapillary RNFL thickness was measured with the high resolution optic nerve head program. With 512 A-scans this program makes a circle with a diameter of 3.4 mm centred on the optic nerve head as shown in figure 1. Only scans with a signal strength ≥5 were accepted. Three consecutive scans were performed and the mean value of the scans was noted. The RNFL thickness is presented in four quadrants, superior, nasal, inferior and temporal, as well as an average thickness for the whole 360°. All scans were performed by one of the authors (UE). Right eyes were examined before left eyes. In the control group one eye from each child was randomised for comparison.13

Optical coherence tomography output for retinal nerve fibre layer thickness of a child in the preterm group.
Statistical methods
Right (RE) and left eyes (LE) were analysed separately and compared with randomised eyes from the control group.13 When comparing prematurely born and full-term children, continuous data were analysed with the Mann–Whitney test or the Kruskal–Wallis test, followed by Dunn's multiple comparison test. As the age at examination differed between prematurely born and full-term children, an ANCOVA model with separate slopes was used in comparisons between the four groups. In the prematurely-born children, Pearson's test for bivariate correlations was used to analyse the relation between RNFL and GA, BW, spherical equivalent and VA. Forward stepwise multiple linear regression analyses were performed to evaluate to what extent the variation in RNFL was explained by GA, BW or severe (stages 3–4) (including treated) ROP (yes/no). A p value <0.05 was considered statistically significant.
Results
Sixty-eight prematurely-born children and 55 controls were initially included in the study.13 The OCT examination could be completed in 62 of the preterm children and 54 of the controls. The qualities of the images were good. The mean signal strength in the control group was 7.7 and in the preterm group 8.7. Descriptive data concerning the groups are presented in table 1. Five of the eight children with severe ROP had been treated. Two of the children in the preterm group had mild ROP in one eye and severe ROP in one eye. There was a significant difference in VA between the groups (p<0.001, RE and LE), but not regarding the spherical equivalent. The mean age at examination was lower in the preterm group (p=0.001), although the range was the same. Gender proportions were similar in the two groups. Eight of the prematurely-born children had known neurological complications (PVL, IVH, CP, epilepsy). Of these eight children, two had previous severe ROP (stages 3–4).
Descriptive data of the preterm group according to stages of retinopathy of prematurity (ROP): no, mild (stages 1–2), severe (stages 3–4) and control group
The mean values for average RNFL thickness in the preterm and full-term children are presented in table 2. There was a significant difference between the study group and the control group regarding RNFL thickness in the superior (RE, p=0.043; LE, p=0.048) and the nasal quadrants (RE, p=0.006; LE, p<0.001), and average RNFL thickness (RE, p=0.016; LE, p=0.029). This difference was caused by a thinner RNFL in children with previous severe or treated ROP (stages 3–4). The differences between the groups remained when age at examination was taken into account in the statistical analyses. Further, we previously found no correlation between age and RNFL in full-term children within the same age span as that of the preterm children in the present study.13 There was no difference between children born at term and prematurely-born children with previous mild ROP (stages 1–2) or without ROP.
Retinal nerve fibre layer (RNFL) thickness in the preterm group according to stages of retinopathy of prematurity (ROP): no, mild (stages 1–2), severe (stages 3–4) and control group
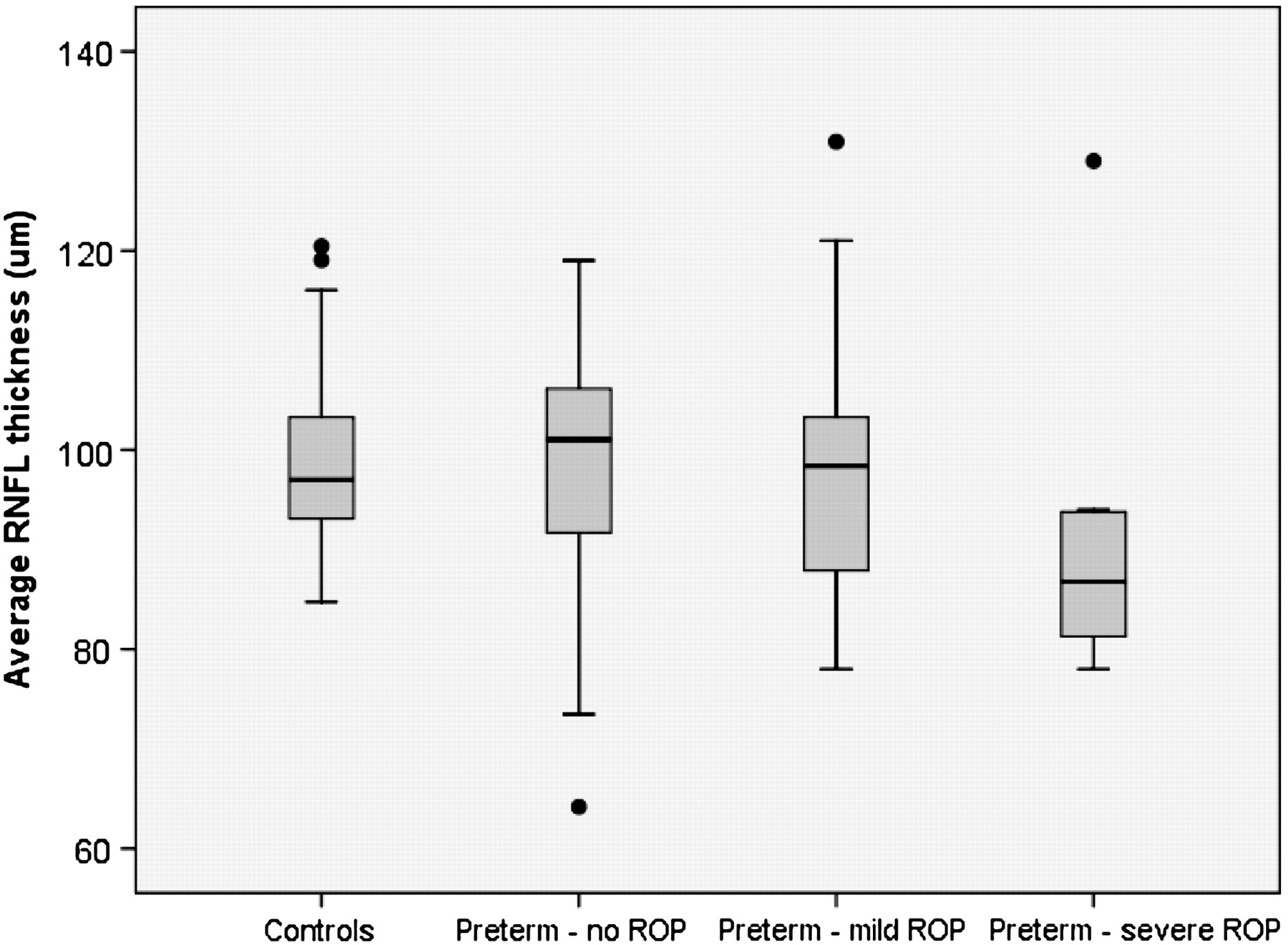
In the prematurely-born group, the average RNFL was reduced in children with previous severe or treated ROP (stages 3–4); see figure 2. No difference was found in average RNFL thickness between the eight children with neurological complications and those without. There were no differences between boys and girls and no correlation between RNFL thickness and spherical equivalent. The average RNFL thickness increased with larger BW (RE, p=0.050; LE, p=0.028), but no correlation with GA at birth was found. In a multiple regression analysis including BW, GA at birth and severe ROP (stages 3–4), the correlation with BW remained significant in LEs (p=0.028), but not in REs. In REs, severe ROP and treated ROP (stages 3–4) were the most significant risk factors for a reduction in RNFL thickness. There was no correlation between average RNFL thickness and VA.

{kind=link}
{kind=link}
Comparison of average retinal nerve fibre layer (RNFL) thickness in the preterm group divided into stages of retinopathy of prematurity (ROP), and the control group.
Discussion
The present study used OCT to evaluate the RNFL in school-aged children who were born prematurely. To our knowledge, such a study has not previously been performed in this group of children. Compared to children born at term, prematurely-born children with severe and treated ROP (stages 3–4) had reduced average RNFL thickness, while children with no ROP or mild ROP (stages 1–2) had no reduction. Within the preterm group, low BW was associated with a reduction in RNFL thickness, but there was no correlation with GA at birth. RNFL thickness did not correlate with VA.
In the present study, the children with severe or treated ROP (stages 3–4) had reduced RNFL thickness. The fact that this group of children has major visual dysfunction has been well described.14 Treatment of ROP most often involves ablation of the peripheral retina with either cryotherapy or laser treatment. This treatment is similar to panretinal photocoagulation (PRP), which is used in patients with proliferative diabetic retinopathy. In a small pilot study, Muquit et al looked at the long-term effect of PRP and found a reduction in average RNFL thickness, suggesting that laser treatment leads to axonal cell death.15 In a larger study by Lim et al, there was a reduction in RNFL thickness in the inferior and nasal quadrants after PRP.16 The results of the present study are in line with the above studies and suggest that cryotherapy/laser treatment for ROP could have the same long-term effect on RNFL thickness as PRP. In addition, severe retinopathy per se might have destructive effects on the ganglion cells. In a recent study by Park et al, RNFL thickness around the optic nerve was assessed in patients with different stages of diabetic retinopathy.17 RNFL thickness was found to decrease with the progression of diabetic retinopathy. Similarly, it may be hypothesised that severe ROP damages the axons of ganglion cells. In the present study, however, the number of children with previous severe ROP (stages 3–4), treated and not treated, was too small to allow sub-analyses of these two groups. Further research, with larger groups of untreated and treated ROP eyes, is needed to elucidate this issue.
Children born prematurely have a higher risk of brain damage, such as IVH and PVL. Recent studies also show that children born preterm have microstructural changes in the brain that are not detected with regular computer tomography or MRI methods.18 Jacobson et al hypothesised that brain damage in prematurely-born children can affect the ganglion cells in the optic nerve and retina by transynaptic retrograde degeneration.19 Eight of the preterm children in the present study had known neurological complications. Unexpectedly, we could not find any reduction in RNFL thickness in these children. Whether the results would have been different in a larger group of children can only be speculated on. In the future, with the development of OCT techniques one might be able to detect more subtle changes, not detected today.
In the present study, there was a correlation between thinner RNFL and lower birth weight. Our results are in accord with two large Australian studies, although the study populations are very different.11 ,12 In a population-based study, the Sydney Childhood Eye Study, a large number of healthy 6-year-old children were examined with OCT; the RNFL thickness was measured, along with several other parameters.11 The authors showed a positive correlation between BW and RNFL thickness, and children with a BW of less than 2500 g had significantly reduced RNFL thickness compared to children with a normal BW. Similar results were shown in the Sydney Myopia Study, where healthy older children were also examined with OCT.12 The retinal ganglion cells start to form the RNFL and optic nerve in the eighth gestational week.20 Between weeks 8 and 18, the retinal ganglion cells increase enormously in number, but at the same time apoptosis reduces the number of axons. Loss of axons is compensated for by increase in glia cells. Wikstrand et al showed that the optic disc neural rim area was smaller in children born preterm and that there were correlations with low birth weight as well as poor postnatal growth.21 They suggested that poor early growth could affect the neural development in this group of children. The results of the present study indicate that the retinal ganglion cells may also be affected by low BW.
In the present study the preterm children had lower VA than children born at term, and this was also the case in a previous population-based study of ours.4 In the study from 2005, children without previous ROP or neurological findings also had reduced VA compared to controls. There may be several explanations, both neurological and retinal, for the reduction in VA in preterm children. In the preterm group of the present study, however, we found no correlation between RNFL thickness and VA. This is in accordance with a recent study of the same cohort, in which we found thicker maculae in the prematurely-born children compared to full-term children, regardless of ROP stage.10 Further, in the preterm group in that study, no correlation between macular thickness and VA was found. Hence, neither of the structural changes measured with OCT, that is, macular thickness and RNFL thickness, could fully explain the subnormal VA of the prematurely-born children in the present cohort.
In conclusion, RNFL thickness was reduced in prematurely-born children with severe or treated ROP (stages 3–4). It could be hypothesised that severe retinopathy per se affects the axons of the neurons, and that the ablation of the retina destroys the neuronal cells. A reduction in RNFL thickness with lower birth weight was also found. Further studies are needed to elucidate the clinical significance of these findings.
Acknowledgments
The authors would like to thank E Berg for statistical advice, and E Nuija and Dr B Schepke for helpful participation in the study.
References
Footnotes
Funding The study was supported by the Crown Princess Margareta Foundation for Visually Impaired, the Mayflower Charity Foundation for Children and the Swedish Society for Medicine.
Competing interests None.
Ethics approval The study was approved by the Ethics Committee in Uppsala, Sweden.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- At a glance