Article Text

Abstract
Background/Aim To determine the preoperative ocular factors and surgical methods that led to best-corrected visual acuity (BCVA) after pars plana vitrectomy (PPV) or scleral buckling (SB) for rhegmatogenous retinal detachment (RRD).
Methods This was a prospective, nationwide, multicentre, observational study. Data from the Japanese Retina and Vitreous Society registry from 2016 to 2017 were used to determine the association between preoperative clinical factors, surgical procedures and postoperative BCVA at 6 months. Japanese individuals >40 years of age were included. Eyes with proliferative vitreoretinopathy were included. The primary outcome was the percentage of eyes that achieved 20/25 vision.
Results Of the 3219 registered cases, 2192 met the inclusion criteria (344 SB, 1738 PPV, 110 PPV+SB). Cases with preoperative BCVA (≤0 logarithm of the minimum angle of resolution (logMAR) units) had good postoperative BCVA (OR=3.97, CI 2.87 to 5.51). Older age (>70 years), low intraocular pressure (<10 mm Hg), high myopia (<−5 dioptres), multiple retinal breaks (>4), giant retinal tear (>90°), wide retinal detachment (>3 quadrants) and macula-off detachment were associated with less probability of postoperative 20/25 vision (OR=0.39, 0.64, 0.62, 0.60, 0.12, 0.51 and 0.36, respectively). Postoperative BCVA was 0.03±0.23 and 0.10±0.32 logMAR units after SB and PPV, respectively. The percentage of cases that achieved 20/25 vision was not significantly different after PPV or SB if cases that had concurrent cataract surgery were excluded (p=0.251).
Conclusions Better BCVA in patients with RRD who had undergone PPV was observed. However, if concurrent cataract surgery is not performed, BCVA will be comparable with either PPV or SB.
- retina
- vision
- treatment surgery
Statistics from Altmetric.com
Introduction
There have been many studies analysing the outcomes of surgery on eyes with rhegmatogenous retinal detachment (RRD). Each report has provided some important information; however, most of the conclusions were based on data collected from a single institution, and the number of cases was relatively small. Because eyes with RRD have different preoperative characteristics that directly affect the outcome, it is necessary to perform a study with a large number of cases to determine the preoperative factors and the best surgical procedures that lead to best visual outcomes.
The registration of clinical cases from multiple sources enables such large-scale investigations. Previous population-based studies include the National Ophthalmology Database study performed in the UK from 2002 to 2010,1 the National Health Insurance Research Database study performed in Taiwan from 1997 to 2005,2 the European VitreoRetinal Society (EVRS) RRD study performed in multiple countries from 2010 to 2011,3 and the Scleral Buckling vs Primary Vitrectomy in RRD (SPR) study performed in Germany from 1998 to 2003.4 To the best of our knowledge, there has not been a prospective large-scale study on the effects of the preoperative factors and type of surgery on the postoperative visual acuity in eyes with RRD using a unified protocol.
The Japanese Retina and Vitreous Society (JRVS) began a registry of all cases of RRD in Japan in February 2016. This registry was called the Japan-Retinal Detachment Registry (J-RD registry). Since its beginning, clinical data have been collected from 3219 Japanese RRD cases from 26 qualified institutions located nationwide between February 2016 and March 2017.
We have investigated the influence of the preoperative characteristics of eyes with RRD on the visual outcome at 6 months postoperatively. In addition, we have compared the postoperative visual acuity at 6 months after scleral buckling (SB), pars plana vitrectomy (PPV) or SB+PPV.
Methods
A detailed report on the study design and procedures for data collection has been published.5 In brief, this registry project collected data of consecutive RRD cases treated at 26 institutions located throughout Japan (see the Acknowledgements section). All of the surgeries were done by vitreoretinal specialists and supervisors certified by the Japanese Ophthalmological Society. The collection of data was through online website dedicated to this study (https://secure2.visitors.jp/retinal_detachment/). The website was open between February 2016 and May 2017. Registration of data was done by individual surgeons. There were more than 50 questions for each case. Postoperative data were collected for up to 6 months after the surgery.
Study participants
Detailed procedures for data collection and the baseline characteristics of the patients are described in detail elsewhere.5 There were 3446 cases submitted with complete information on preoperative characteristics and surgical procedures. Two hundred and twenty-seven cases were excluded because they had undergone previous surgeries for RRD. Cases with macular holes, posterior breaks and vitreous haemorrhage were also excluded because all of them had very poor preoperative visual acuities. The exclusion of these cases was determined by the JRVS registry committee members: TB, RK, KY, TK, KN and TS. Patients younger than 40 years were excluded because they had a unique characteristic of the absence of vitreous detachment and were usually treated by SB. In the end, 2192 (63.6%) cases were used for statistical analyses.
Data collection
The questionnaire about the clinical characteristics before surgery and surgical interventions was developed by the JRVS registry committee members based on previous reports.3 6 7 The results were collected by standardised web-based electronic data capture system. The active JRVS members who were experienced ophthalmologists, with an experience of treating >50 RRD cases/year, registered their data manually. The information collected included age at time of surgery, sex, interval between diagnosis and surgery (0, 1–3, 4–7, 8–13, 14–28 or 29+ days), best-corrected visual acuity (BCVA) at baseline in logarithm of the minimum angle of resolution (logMAR) units, intraocular pressure (IOP, 0–10, 11–12, 13–14 or 15+ mm Hg), refractive error (spherical equivalent (dioptre): <−10 D, −10 D to <−5 D, −5 D to <−1 D, −1 D to <+1 D, +1 D to <+5 D, or ≥+5 D), axial length (<22.0, 22.0–26.0 or >26.0 mm), lens status (aphakia, phakia or pseudophakia), type of retinal tears/holes (atrophic holes, tears, or breaks at or near the vitreous base), number of tears or holes (1, 2–3 or 4+), location of the largest tears or holes (superior-temporal, superior-nasal, inferior-temporal, inferior-nasal or the posterior pole), size of the largest tear or hole (0°–30°, 30°–60°, 60°–90° or 90°+), area of detachment (1–4 quadrants), presence of macular detachment, duration of macular detachment (based on the patient’s symptoms), choroidal detachment, hypotony (IOP <5 mm Hg), and presence of proliferative vitreoretinopathy (PVR; N/A, B or C).
PPV was the most common procedure (1738, 79%), followed by SB (344, 16%) and PPV+SB (110, 5%). During the time of this registry, 99.5% of PPV procedures used microincision vitrectomy (MIVS) with the use of 23G, 25G and 27G systems. The lower visual acuities of no light perception was graded as 4.0 logMAR units, light perception 3.0 logMAR units, hand motion 2.3 logMAR units and counting fingers 2.0 logMAR units, as reported by Schulze-Bonsel et al.8
Clinical information collected after surgery
Clinical data on the surgical procedures and postoperative findings including complications were collected at 1, 3 and 6 months postoperatively, as described in detail.5 Any additional surgical procedures were also recorded.
Definition of primary success and failure levels
Primary success was defined as having no additional surgery during the 6 postoperative months. Silicone oil removal was planned within 6 months if no other additional procedures were required. The surgery to remove silicone oil was not counted as an additional surgery. Definitions of level 1–3 failures were adopted from studies by the EVRS study.3 6 7
Statistical analyses
We first determined whether there were significant correlations between baseline BCVA and presurgical clinical characteristics of patients. We included covariates of age, time to surgery, IOP, refractive error (spherical equivalent), axial length, lens status, type of tears/holes, number of tears/holes, location of the largest tears/holes, size of the largest tears/holes, area of detachment, macular detachment, choroidal detachment, hypotony, PVR category and type of surgical procedure.
Second, we determined the association between failure levels and BCVA at 6 months. Postoperative BCVA was analysed separately for eyes treated by SB, PPV or PPV+SB. The average BCVA at 6 months and the probability of achieving a BCVA of 0.1 logMAR units (20/25) were calculated according to the type of surgery.
Third, we used mixed linear regression models to estimate the OR associated with the average BCVA at 6 months with a random intercept considering the correlation within clinic level and hospital level. We modelled for overall patients treated with SB or with PPV separately. In the models, we included covariates of age, time to surgery, IOP, refractive error, axial length, lens status, type of tears/holes, number of tears/holes, location of the largest tears/holes, size of the largest tears/holes, area of detachment, macular detachment, choroidal detachment, hypotony and PVR category.
Finally, we compared the odds of achieving good BCVA of 0.1 logMAR units (20/25) or better at 6 months. We estimated the association adjusting for potential confounding factors, both associated with preoperative visual acuity and outcome. We determined the interactions for the significant determinants indicated in the models for achieving a BCVA of 0.1 logMAR at 6 months.
All analyses were conducted with Stata V.16.0, and a p value of <0.05 was considered statistically significant.
Results
Of the 3446 total cases in the registry, 2192 were found to meet the inclusion criteria (online supplementary table S1).
Supplemental material
Characteristics that affected baseline BCVA
The factors associated with poor baseline BCVA were older age, low IOP of <10 mm Hg, refractive error <−10 D and greater than +1 D, eyes with an intraocular lens, flap tears especially breaks near the ora serrata, multiple retinal breaks, that is, more breaks associated with worse vision, breaks located at the superior temporal quadrant, retinal detachment (RD) of more quadrants, macular detachment, choroidal detachment, hypotony, and high PVR grade. On the other hand, sex and size of the breaks were not significantly associated with poor baseline BCVA (online supplementary table S1). These clinical characteristics that were significantly associated with poor vision were similar if the population with good vision of ≥0.1 logMAR units was used to assess the relationships (online supplementary table S2).
Supplemental material
Levels of failure and BCVA at 6 months
In this registry, the overall primary success was 90.8%; primary success in cases treated with SB was 93.1%, PPV was 91.8% and PPV+SB was 68.7%. The details are being reported elsewhere. The cases successfully treated by the initial surgery had better BCVA than the cases treated by multiple surgeries for both SB and PPV surgeries. The cases with a postoperative vision of ≥0.1 logMAR units had the same trend after SB or PPV (table 1). The cases with a high level of failure had poorer postoperative BCVA and lower possibility of achieving a BCVA of 0.1 logMAR units in cases treated by PPV alone. None of the cases treated by SB had level 3 failure cases but had the same trend (table 1).
BCVA by surgical outcome at 6 months
The visual outcomes had the same trend in the cases treated by PPV+SB, although these RRD cases might have had more complex backgrounds (table 1).
Baseline factors which affected BCVA at 6 months in cases treated with PPV alone or with PPV + cataract surgery
We analysed the visual outcomes of eyes that had undergone concurrent cataract surgery with the RRD surgery separately because the concurrent cataract surgery can affect 6-month BCVA (online supplementary table S3). The worst BCVA at 6 months was found in eyes that had poor baseline BCVA, older patients, IOP <10 mm Hg, refractive error <−5 D, multiple retinal breaks with breaks located in the superior temporal quadrant, breaks >90°, RD >3 quadrants and macula-off RD (online supplementary table s3, model 1). On the other hand, sex, axial length, type of retinal breaks, presence of choroidal detachment and degree of PVR were not significantly associated with BCVA at 6 months. After adjusting for these associations, the probability of achieving a BCVA of 0.1 logMAR units at 6 months was better in the eyes treated by PPV than by SB (OR=1.75, 95% CI 1.18 to 2.58; p=0.005).
Supplemental material
Among all eyes treated by PPV, the eyes that had undergone concurrent cataract surgery had a greater positive influence on BCVA at 6 months (OR=2.89, 95% CI 1.69 to 4.94; p<0.001; figures 1 and 2). Therefore, we excluded the PPV cases with cataract surgery in the following statistical analyses. We did not have any cases that had to undergo cataract surgery during the 6-month follow-up period. Although the grades of the cataract were not included in the registry data, we can assume that severe progression of cataract did not occur in the cases which were treated without concurrent cataract surgery.

Graph showing the changes in best-corrected visual acuity (BCVA) in cases with macula-on rhegmatogenous retinal detachment. The cases treated by scleral buckling (SB) have decreased BCVA postoperatively but then returned to the baseline value. The cases treated by pars plana vitrectomy (PPV) had a significant improvement at 1 month postoperatively. PPV alone improved BCVA to 0.1 logMAR units (20/25). The trend is more obvious in cases treated by concurrent PPV and cataract surgery. logMAR, logarithm of the minimum angle of resolution.

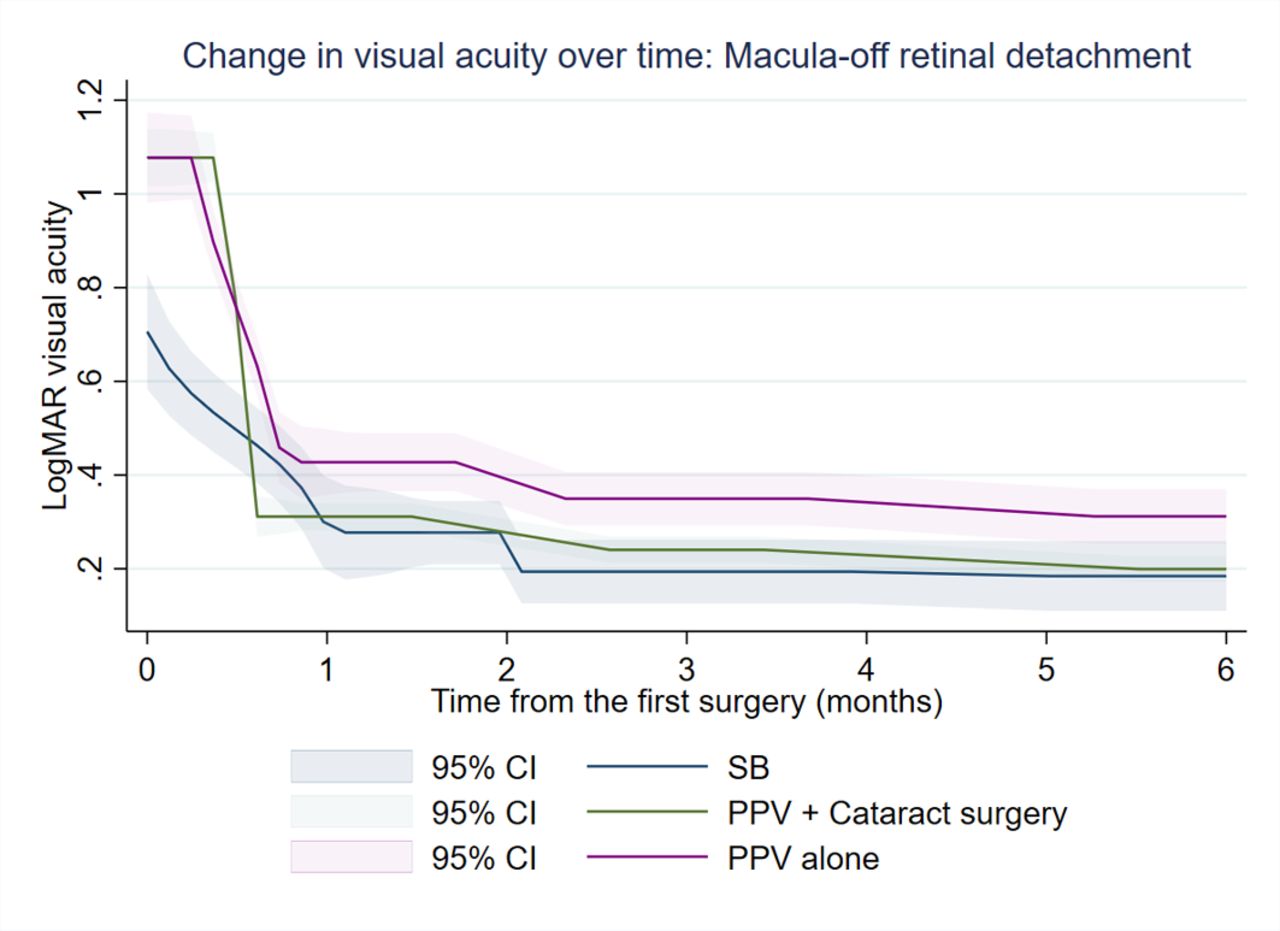
Graph showing changes in best-corrected visual acuity (BCVA) in cases with macula-off rhegmatogenous retinal detachment preoperatively. Visual recovery is observed within 1 month in cases treated by either scleral buckling (SB) or pars plana vitrectomy (PPV). BCVA was stable after 1 month in the postoperative period. There was no significant difference in BCVA at 6 months between the cases treated by SB, PPV + cataract surgery, and PPV alone. logMAR, logarithm of the minimum angle of resolution.
Baseline factors that were significantly correlated with BCVA at 6 months after PPV with and without cataract surgery (online supplementary table S3, model 2)
The negative association between the baseline characteristics of older patients, IOP <10 mm Hg, refractive error <−5 D, multiple retinal breaks located in the superior temporal quadrant, breaks >90°, RD >3 quadrants and macula-off RD and BCVA at 6 months, which was significant in model 1 (with or without cataract surgery), was not significant in model 2 (without cataract surgery). In addition, the differences between SB and PPV in the cases that had BCVA of 0.1 logMAR units at 6 months were not significant (OR=0.89, 95% CI 0.51 to 1.54; p=0.251).
Association between baseline characteristics and BCVA at 6 months in cases treated by PPV
Finally, we analysed the association between preoperative factors and postoperative BCVA in the cases treated with PPV alone (online supplementary table s4, model 3). The baseline factors associated with poor BCVA at 6 months were poor baseline BCVA, older age especially >70 years, hyperopia of +1 D and +5 D, breaks >90°, RD >3 quadrants, macula-off RD and use of silicone oil (SO). The eyes with simultaneous cataract surgery had better BCVA at 6 months.
Supplemental material
To confirm the poor visual prognosis in the elderly, we analysed the cases treated within 1 week of the onset and found that the final BCVA was poorer as the patient’s age increased (online supplementary table S5).
Supplemental material
Discussion
The cases that had successful primary surgery (level 0) had better final BCVA and higher rate of achieving a BCVA of 0.1 logMAR units regardless of the type of surgery. Thus, primary surgery resulted in good vision. Visual prognosis became worse when a reoperation was needed (failure level 1), use of SO tamponade (level 2) and when detached areas remained (level 3). The cases with level 2 failure (SO tamponade) had an average vision of 0.57 logMAR units after PPV and 0.74 logMAR units after PPV+SB. This indicates that the level 2 group may have included cases with macular atrophy and residual detachment.
Among the most important factors that had negative effects on preoperative BCVA were older age and lower IOP. Factors that delayed the time of diagnosis9 in elderly patients with RD were impaired macular function10 and presence of cataract.11 When the patients who were treated within 1 week of the diagnosis were analysed, postoperative BCVA was still poor (online supplementary table S5). This suggests a negative influence of potentially low macular function associated with ageing. Macular function can be impaired by choroidal dysfunction in cases with hypotony.12 Liquefaction of the vitreous gel is more likely to be present in older individuals, and the detachment rapidly involves the macula. In addition, these eyes are likely to become hypotonic.13 14
Our findings of the significant effects of poor baseline visual acuity on postoperative visual acuity confirmed those in earlier reports.15 The cases with multiple quadrants of detachment and breaks at the superior temporal area seem to develop macular detachment and had poor visual outcome. In pseudophakic eyes, the cases with an inferior break had poor visual outcome.15 On the other hand, our results showed that superior breaks had negative effects on postoperative BCVA. In the SPR study, the incidence of inferior breaks was extremely low (4.7%, 32 of 680 eyes), and a few cases with very poor vision decreased the average visual outcome. In our registry, inferior breaks were observed in 23.2% (508 of 2191) of cases, and therefore we were able to evaluate the impact of the location of breaks more accurately.
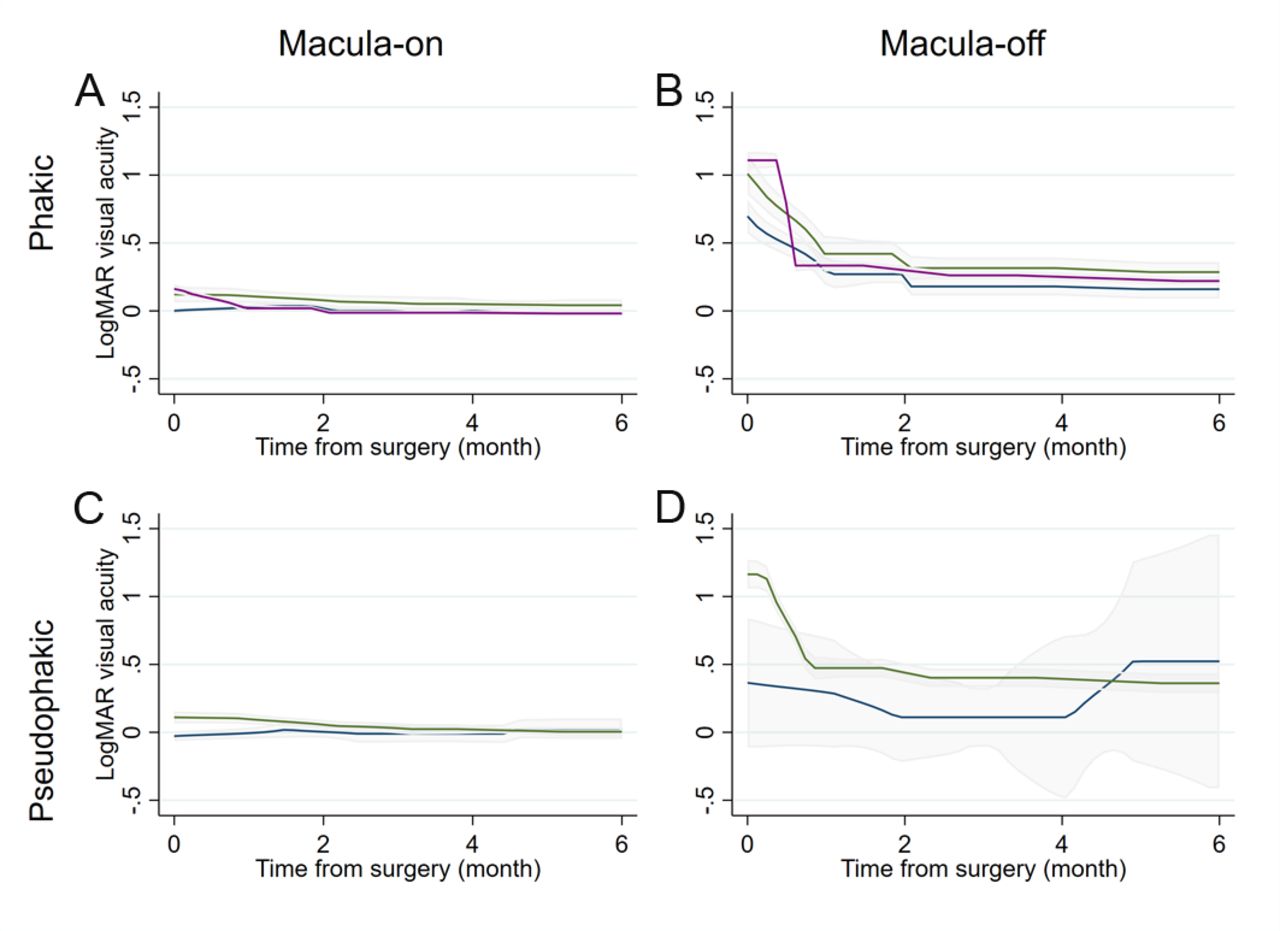
Our results showed that postoperative visual acuity was highly dependent on whether the macula was detached and whether cataract surgery was conducted simultaneously. These findings are shown in figure 3, showing the effects of SB, PPV without simultaneous cataract surgery, and PPV with simultaneous cataract surgery in eyes with macula-on or macula-off RD. As shown, postoperative visual acuity at 6 months seems most influenced by simultaneous cataract surgery in phakic eyes. There was no significant difference in pseudophakic eyes between SB and PPV. When the multivariate model was confined to pseudophakic eyes and compared SB or PPV, there was no significant difference in visual acuity at 6 months in the multivariate model (overall p=0.477). When we confined the analysis to phakic eyes, the odds of achieving good vision were marginally higher in eyes treated by PPV with cataract surgery than eyes that underwent SB (adjusted OR 1.44; p=0.111), while eyes treated by PPV without cataract surgery had a significant negative association (adjusted OR 0.43; p=0.008). This also supports our overall observation that postoperative BCVA was affected by concurrent cataract surgery, and the eyes treated by PPV with concurrent cataract surgery had better visual outcome than SB alone. Generally, the final BCVA in our cohort (figure 3) was better than that reported by Heimann et al 4 (SB=0.33 logMAR units and PPV=0.48 logMAR units in phakic eyes, p=0.0005; SB=0.46 logMAR units and PPV 0.38=logMAR units in pseudophakic and aphakic eyes, p=0.1033). In another report, SB resulted in a BCVA of 0.5 logMAR units, PPV resulted in 0.7 logMAR units and PPV+SB in 1.1 logMAR units (p=0.73).1 The influence of cataract surgery was not taken into account in these earlier studies. Thus, these findings indicated that information on concurrent cataract surgery should be assessed when BCVA is investigated after PPV for RD. When analysis was confined to patients aged 40–49 years, there was no significant association observed (p=0.381). This subanalysis however was not definitive and a large number of patients are needed to determine whether there is a significant association in younger patients.
{kind=link}
{kind=link}
{kind=link}
Graph showing change in best-corrected visual acuity (BCVA) in phakic and pseudophakic eyes treated by scleral buckling (SB) and pars plana vitrectomy (PPV) with or without cataract surgery. (A) BCVA after SB (blue) and PPV with (red) or without (green) concurrent cataract surgery in phakic eyes with macula-on rhegmatogenous retinal detachment (RRD). BCVA in cases after PPV with cataract surgery was not significantly different from cases after SB and was better than cases after PPV without concurrent cataract surgery. (B) BCVA after PPV with cataract surgery in the phakic, macula-off RRD was better than that after PPV without cataract surgery. (C) BCVA in the pseudophakic, macula-on eyes after PPV and SB was comparable. (D) BCVA in the pseudophakic, macula-off eyes with PPV was better than that after SB at 6 months postoperatively. logMAR, logarithm of the minimum angle of resolution.
In the eyes with a macula-on detachment, BCVA improved by 0.1 logMAR units after PPV without cataract surgery. An earlier study showed that macular electroretinograms (ERGs) were reduced even in the eyes with macula-on detachment.16 The changes of the cytokines in the vitreous or a recovery of the retinal ischaemia may be the cause of the improvement of macular function.
Visual outcomes may be poorer because eyes with a giant retinal break are at a higher risk of unsuccessful surgery. An improvement in BCVA was observed in only 18%–37% of the cases treated by PPV combined with SB.17–19 The eyes with preoperative poorer BCVA15 and macula-off RD20 had a negative effect on postoperative BCVA, as reported.
SO is usually used for complicated cases that have poor prognosis. In addition, SO has been reported to make the inner retina thin and reduce visual function during the period of the tamponade.21 These factors may explain the poorer postoperative BCVA in these eyes with SO tamponade.
Posterior vitreous detachment (PVD) was observed in 67.8% of the cases treated by SB and 90.5% of the cases treated by PPV. The diagnosis of PVD was accurate in the cases treated by PPV because it was confirmed during the surgeries. However, the diagnosis of PVD was not as reliable in the cases treated by SB, and therefore we did not include the PVD status in our analyses.
There are limitations to this study. The definition of the duration of macular detachment was an estimation based on symptoms and clinical interviews. Because it is not possible to review the macular detachment status in a standardised manner, this duration needs to be accepted with some reservations. However, in a clinical setting, the estimation of macular detachment is commonly used, and this might be a simple clinical indicator that can provide prognostic information on whether there is an association between duration of macular detachment and visual outcome. Another limitation was that some cases lacked information on postoperative BCVA, and these cases had to be excluded. In addition, there were missing data for some of the key parameters including axial length (421 missing). This might be a random error; however, there is a potential for systematic errors or a selection bias of having mild or simple RD being included in the analyses. Also, the preoperative grade of cataract was not included in the registry even though our results showed the importance of concurrent cataract surgery in improving postoperative vision. The designation of BCVA in eyes with very poor vision has not been definitively set and we had to use an approximation. The selection of surgery type was made according to the surgeon’s experience. We used random intercept considering correlation within the clinic/hospital level and minimised the bias associated with the facilities.
In conclusion, we investigated the visual outcome after treatment for RD cases by the standard type of surgery performed in Japan during the study period. We found that 99.5% of PPV procedures were performed with MIVS, and the visual outcome was still comparable between PPV and SB. This is the first report describing postoperative BCVA based on a detailed analysis of a large number of Japanese RD cases. The results showed comparable visual outcomes at 6 months regardless of type of surgery, SB and PPV if we exclude the effect of cataract surgery in the cases treated by PPV. Although the current standard of care for RD has a trend of increasing use of PPV, SB is still useful with the same level of visual recovery as PPV.
References
Footnotes
Presented at Part of these data was presented at the XXXIth Meeting of the Club Jules Gonin, Jersey, Channel Islands (GB) and the Vail Vitrectomy, Vail, Colorado, 2019.
Contributors Conception and design: TB, RK. Data collection: TB, KY, TK, KN. Analysis and interpretation: TB, RK, TS. Obtained funding: SY, TS. Overall responsibility: TB, RK, KY, TK, KN, SY, TS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests TB reports personal fees from Bayer Yakuhin, personal fees from Kowa, personal fees from Santen, personal fees from Senju, grants and personal fees from Novartis Pharma KK, personal fees from Alcon Japan, outside the submitted work. RK reports personal fees and other from Topcon, grants and personal fees from Senju, grants and personal fees from Novartis Pharma KK, grants from Pfizer, grants and personal fees from Bayer Yakuhin, personal fees from Roche, personal fees from Takeda, personal fees from Kowa, personal fees from Novo Nordisk, personal fees from Astellas, personal fees from Santen, personal fees from Nitto Medic, personal fees from Office Future, personal fees from Predictive Analytics, personal fees from MICIN, outside the submitted work. KY reports personal fees from Bayer Yakuhin, personal fees from HOYA Corporation, personal fees from Novartis Pharma KK, personal fees from Alcon Japan, personal fees from RE Medical, outside the submitted work. TK reports personal fees from Santen, personal fees from Bayer Yakuhin, personal fees from Novartis Pharma KK, personal fees from HOYA Corporation, personal fees from Ellex, personal fees from Pfizer, personal fees from Kowa, personal fees from Senju, outside the submitted work. KN reports personal fees from Santen, personal fees from RE Medical, personal fees from Carl Zeiss, personal fees from Alcon Japan, personal fees from Novartis Pharma KK, personal fees from Kowa, personal fees from Johnson & Johnson, personal fees from Senju, personal fees from Sanwa Kagaku Kenkyusho, personal fees from HOYA Corporation, outside the submitted work. SY reports grants and personal fees from Santen, grants and personal fees from Jamecs, personal fees from HOYA Corporation, personal fees from Pfizer, personal fees from Senju, personal fees from Alcon Japan, personal fees from Nidek, personal fees from Kowa, personal fees from Bayer Yakuhin, outside the submitted work. TS reports personal fees from Bayer Yakuhin, personal fees from HOYA Corporation, personal fees from Novartis Pharma KK, personal fees from Alcon Japan, personal fees from RE Medical, personal fees from Santen, personal fees from Senju, outside the submitted work.
Patient consent for publication Not required.
Ethics approval The main study protocol was approved by the Ethics Committee of Kagoshima University (140093 (28-38)), and all the facilities thereafter and the procedures used conformed to the tenets of the Declaration of Helsinki. The collection of data was conducted based on the Ethical Guidelines for Medical and Health Research Involving Human Subjects in Japan (https://www.mhlw.go.jp/file/06-Seisakujouhou-10600000-Daijinkanboukouseikagakuka/0000080278.pdf).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information. Data from the J-RD database are available upon reasonable request.
Linked Articles
- At a glance