Article Text

Abstract
Purpose To evaluate the effects of 0.01% and 0.02% atropine eye drops on myopia progression, pupil diameter and accommodative amplitude in myopic children.
Methods A cohort study assessed 400 myopic children divided into three groups: 138 and 142 children were randomised to use either 0.02% or 0.01% atropine eye drops, respectively. They wore single-vision (SV) spectacles, with one drop of atropine eye drop applied to both eyes once nightly. Control children (n=120) only wore SV spectacles. Repeated measurements of spherical equivalent refractive errors (SERs), axial length (AL), pupil diameter and accommodative amplitude were performed at baseline, and 4, 8 and 12 months after treatment.
Results After 12 months, the SER change was −0.38±0.35D, −0.47±0.45D, −0.70±0.60D and AL change was 0.30±0.21 mm, 0.37±0.22 mm, 0.46±0.35 mm in the 0.02%, 0.01% atropine and control groups, respectively. There were significant differences in the change in AL and SER between three groups (all p<0.001). Between baseline and the 12-month visit, the overall change in accommodative amplitude was 1.50±0.25D, 1.61±0.31D and change in pupil diameter was 0.78±0.42 mm, 0.69±0.39 mm, with 0.02% and 0.01% atropine, respectively. Accommodative amplitude significantly decreased and pupil diameter significantly increased in two atropine groups (all p<0.001). Moreover, there was no statistical difference in the change difference in accommodative amplitude and pupil diameter between two atropine groups (p=0.24, p=0.38), whereas the accommodative amplitude (p=0.45) and pupil diameter (p=0.39) in the control group remained stable.
Conclusions 0.02% atropine eye drops had a better effect on myopia progression than 0.01% atropine, but 0.02% and 0.01% atropine showed similar effects on pupil diameter and accommodative amplitude after 12 months of treatment.
Trial registration number ChiCTR-IPD-16008844.
- drugs
- clinical trial
- child health (paediatrics)
- optics and refraction
Statistics from Altmetric.com
Introduction
The increasing prevalence of myopia and high myopia has significant economic and social impacts.1 2 Currently, multiple methods are used to control the progression of myopia, including low-dose atropine eye drops,3–7 orthokeratology (OK) lens,8 peripheral defocus contact lenses,9 increased outdoor activity10 11 and sunlight exposure time.12 Currently, OK lens use is the most common approach to slowing down myopia progression in mainland China. OK lens wear temporarily reduces the degree of myopia and controls the speed of myopia progression.8 13 14 However, some myopic children do not fully benefit from this approach because of individual differences in the response to OK lens,15 decreased visual quality,16 the limited range of refractive correction available and the strict compliance expectations for successful OK lens wear.
At present, another effective method to control myopia progression in children is atropine eye drop administration.17 Atropine has a dose-related effect on myopia progression with greater effect and more obvious side effects, including photophobia, poor near vision and rebound effects after cessation, seen with higher doses.5 All these risks appear to be substantially mitigated by the administration of low atropine concentrations. Many studies have shown that moderate and low concentrations of atropine (eg, 0.01%, 0.025%, 0.05%, 0.1%) could control the progression of myopia in children with reasonable efficacy, minimal side effects, convenient use and slight rebound effects after discontinuation.4–6 17 However, there are differences in the efficacy and side effects (reduction in amplitude of accommodation pupil dilation and symptoms such as photophobia and near blur vision) with different concentrations of low-dose atropine.5 7 18 Yam et al7 and Moon and Shin19 found that different atropine doses had different myopia progression effects with administrations of 0.01%, 0.025% and 0.05% atropine, but the dose-dependent side effects were only in Yam et al’s study,7 but not in Moon and Shin’s study.19 Moreover, Chia et al5 found that 0.01% atropine had minimal side effects compared with 0.1% and 0.5% atropine, but there was no difference in the myopia progression effect between 0.01% and 0.1% atropine.
This study involved a 1-year longitudinal study in Central China with children randomised to either 0.02% and 0.01% atropine or to wear single-vision (SV) spectacles only. Myopia progression efficacy and effects on amplitude of accommodation and pupil diameter were explored.
Methods
Four hundred right eyes of Chinese myopic children (Han nationality) who visited the First Affiliated Hospital of Zhengzhou University were recruited into this cohort study between June 2016 and June 2017. The inclusion criteria were: 6–14 years of age, spherical equivalent refractive error (SER) from −1.25 to −6.00D, astigmatism less than 2.0D, anisometropia of less than 1.0D, monocular best-corrected visual acuity of 16/20 or better, intraocular pressures (IOP) between 10 and 21 mm Hg, and no other eye diseases and surgery. Exclusion criteria were previous use of atropine, pirenzepine, rigid gas-permeable and OK lens to control myopia progression, and inability to comply with the study visit schedule.
At the randomisation visit, eligible subjects were given the option of atropine or no atropine, per human ethics committee of requirements, and the atropine groups were subsequently assigned in a double-blinded and randomised manner either to 0.01% or 0.02%. This study conformed to the tenets of the Declaration of Helsinki. Possible risks were fully explained before treatment initiation. The experimental drug (1% atropine eye drops; Eye and ENT Hospital Affiliated to Fudan University) was diluted with saline (also added ethyl hydroxybenzoate) to 0.01% or 0.02% on a clean bench (3 mL sealed bottle, 15–25°C room temperature storage, discarded eye drops after opening the bottle for 1 month).
Children were reassessed at the 1-month monitoring visit after starting atropine and then at 4, 8 and 12 months. At each visit, all examinations were performed by the same clinician who was masked to the experimental group of each subject. The children in the control group were prescribed full-correction, SV spectacles with the highest positive/least negative power consistent with optimum visual acuity, for constant wear. The two experimental groups wore the SV spectacles prescribed under the same protocol as the control group and administered one drop of atropine eye drops into both eyes once nightly before bed time.
Pupil diameter was measured using an autorefractor (NIDEK, AR-1, Japan) when looking at a distant target with no refractive correction under indoor light. The lighting level was kept constant with an illumination of 300 to 310 lux (TES-1332A Illumination photometer). Children were adapted to ambient light for 10 min in the examination room before taking measurements. On each occasion, three successive measurements were made, and average values were recorded. The right eye was assessed before the left. Accommodative amplitude was measured monocularly by the push-up technique. The children wore their fully corrected spectacle prescription and focused on the previous line of best-corrected visual acuity with the right eye while the left one was occluded. The children were instructed to focus on a letter as the chart was moved closer. They were told to keep the letter as clear as possible until it could no longer be held in clear focus. The inverse of the final distance in metre was recorded as the child’s accommodative amplitude. Accommodative amplitude was recorded three times and the average taken. Corneal power, anterior chamber depth (ACD) and axial length (AL) were evaluated using a non-contact partial coherence interferometer (IOLMaster; Carl Zeiss Meditec AG, Germany). On each occasion, five successive measurements were taken and their mean was used for analysis. Cycloplegic autorefraction was performed after the instillation of four drops of compound tropicamide eye drops (0.5% tropicamide and 0.5% neo-synephrine) (Santen, Japan) administered 10 min apart in each of the patients’ eyes. Ten minutes after the instillation of the fourth drop, three autorefraction measurements were taken (Topcon RM 8000A, CA) and a mean was obtained. The degree of myopia is expressed as SER.
Discomfort symptoms in the experimental groups were assessed using a paper questionnaire at each follow-up visit. Based on questionnaires used in previous studies,18 20 our questionnaire included three groups of questions: (1) How often are you experiencing aversion to light? (never, occasionally, often, always); how severe is the aversion to light? (zero, normal indoor, daily outdoor, bright sun light); (2) How often do you experience blurred vision at near? (never, occasionally, often, always); how severe is the blurred vision at near (zero, mild, moderate, severe) and the duration? (3) How often do you experience the itchy eyes, eye swelling and other discomforts (never, occasionally, often, always); how severe is the itchy eyes, eye swelling, other discomforts (zero, mild, moderate, severe) and the duration? The clinical examinations and symptoms questionnaire were conducted in the morning.
Continuous baseline variables were expressed as mean±SD and evaluated by analysis of variance. Categorical variables, such as sex and parental myopia status, were expressed as percentage (%) and evaluated by the χ2 test. The 1-month monitoring data for AL and SER was compared with baseline using t test to explore whether an initial hyperopic shift was evident. A generalised additive mixed model was used to estimate the longitudinal trend with time (baseline, 4 months, 8 months and 12 months) for dependent variables (SER, AL, pupil diameter and accommodative amplitude) and differences in rate of change between the three groups. The change represents the slope for each treatment group of dependent variables over time, and the change difference represents the difference in slope of dependent variables over time between groups. A p value <0.05 was considered statistically significant. All statistical analyses were performed using Empower (www.empowerstats.com; X & Y Solutions, Boston, MA) and R (http://www.R-project.org).
Results
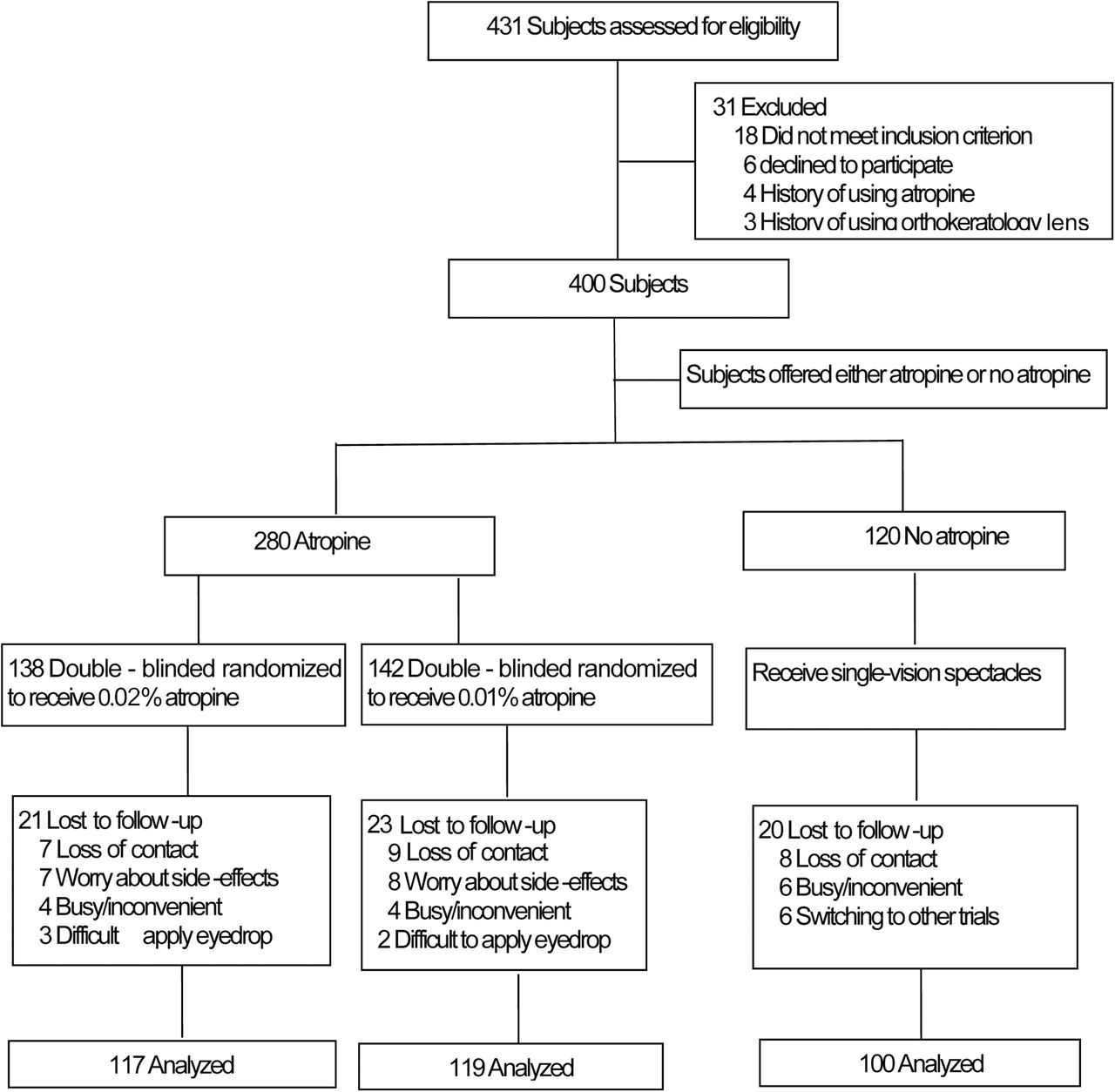
A total of 400 children were enrolled in this cohort study. There were 138, 142 and 120 children in 0.02% atropine, 0.01% atropine and control groups, respectively (figure 1). No differences were found in age, sex, body mass index, parental myopia status, IOP, pupil diameter, accommodative amplitude, ACD, corneal curvature, SER and AL between groups (table 1). Of the 400 children enrolled, 336 successfully completed the 12-month follow-up examinations. Sixty-four subjects (16%) dropped out, including 21 (15.2%), 23 (16.1%) and 20 (16.6%) in the 0.02% atropine, 0.01% atropine and control groups, respectively. There were no significant differences in baseline parameters between the drop-out subjects and those who completed the study (p>0.05).
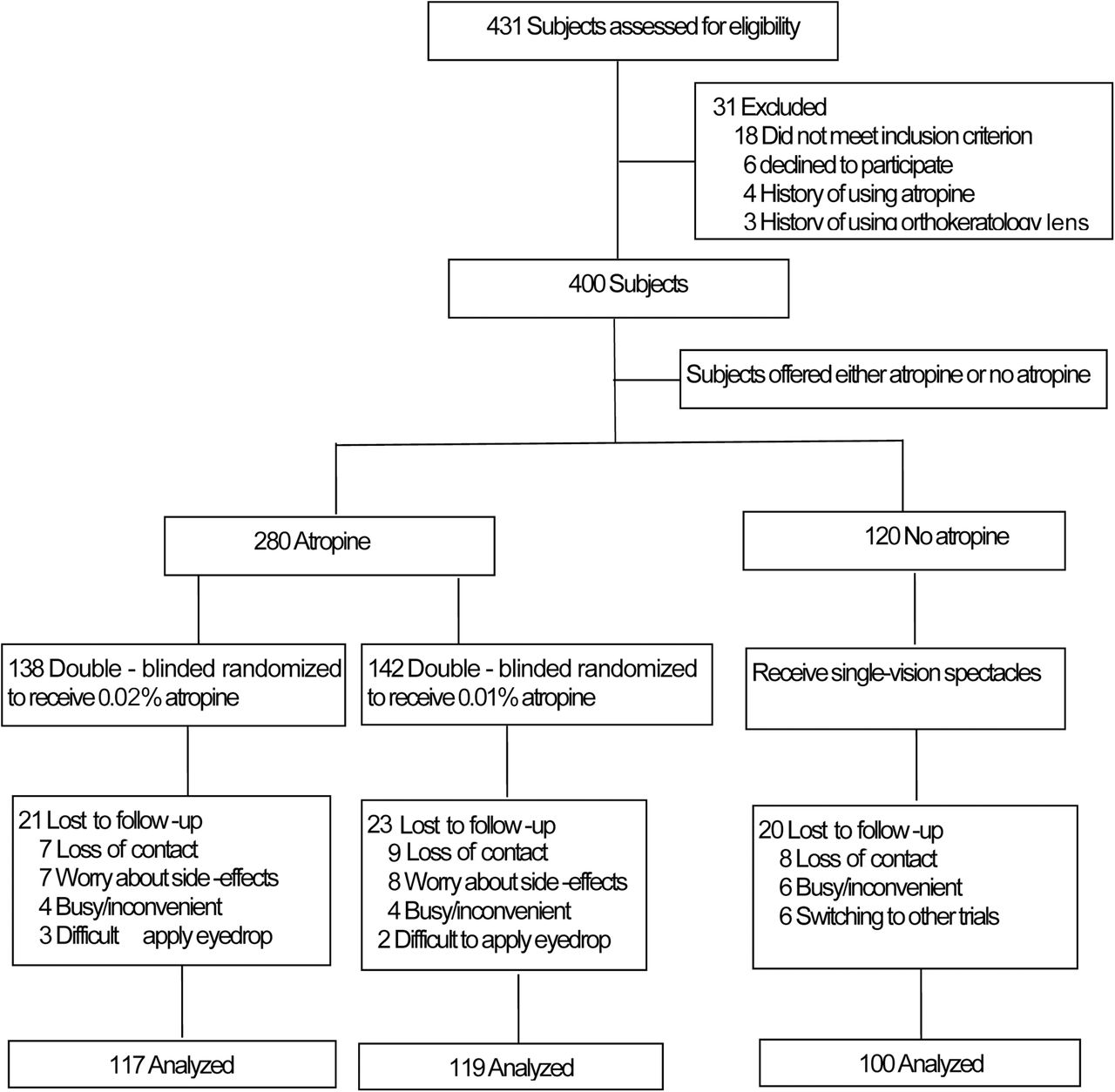
Subject recruitment and randomisation flowchart.
Baseline characteristics of study participants
The SERs before and 1 month after medication were −2.76D, −2.70D, −2.68D and −2.80D, −2.76D, −2.75D; the ALs before and 1 month after medication were 24.60 mm, 24.58 mm, 24.55 mm and 24.65 mm, 24.62 mm, 24.62 mm in 0.02%, 0.01% atropine and control groups, respectively. At the 1-month monitoring visit, there was no initial hyperopic shift and AL shortening compared with baseline in the three groups (all p>0.05).
An atropine concentration-dependent response was observed for myopia progression. At the end of 1 year, SER change was −0.38±0.35D, −0.47±0.45D, −0.70±0.60D and AL change was 0.30±0.21 mm, 0.37±0.22 mm, 0.46±0.35 mm in the 0.02%, 0.01% atropine and control groups, respectively. There was a significant increase shown in change in SER from baseline to 12 months in three groups (all p<0.001; figure 2 and table 2). The changing trend of change in AL was the same as the change in SER in three groups (all p<0.001; figure 3 and table 2).

Measurement of spherical equivalent refractive error over time.

Measurement of axial length over time.
Change and change difference of SER and AL in three groups over 1 year*
In total, 50.2%, 45.1% and 28.1% of subjects progressed by less than 0.5D in the 0.02%, 0.01% atropine and control groups, respectively, whereas 16.7%, 20.3% and 35.6% subjects progressed by more than 1.0D in the 0.02%, 0.01% atropine and control groups, respectively.
There was no dose-dependent response to atropine in accommodative amplitude and pupil diameter change in the atropine-treated groups. Compared with baseline, accommodative amplitude significantly decreased at 4 months in 0.02% and 0.01% atropine groups (all p<0.001; figure 4 and table 3). Then, there was a slight upward trend at 8 and 12 months. Pupil diameter significantly increased in 0.02% and 0.01% atropine groups (all p<0.001; figure 5 and table 3). There was no statistical difference in the change difference of pupil diameter between two atropine groups from baseline to 4 months (p=0.55). Pupil diameter then remained stable from 4 months to 12 months in both treatment groups. From baseline to 12 months, the overall change in accommodative amplitude (p=0.24) and pupil diameter (p=0.38) was not significantly different between 0.02% and 0.01% atropine, whereas the accommodative amplitude (p=0.45) and pupil diameter (p=0.39) in the control group remained stable over time (figures 4 and 5 and table 3).

Measurement of accommodative amplitude over time.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Measurement of pupil diameter over time.
Change and change difference of accommodative amplitude and pupil diameter in three groups over 1 year*
Thirty-two (23%, 0.02% atropine) and 33 (24%, 0.01% atropine) children were photophobic in bright sunlight, but no other discomfort in normal indoor or daily outdoor light was experienced in either atropine group. Photophobia was resolved by wearing sunglasses or sun hats during outdoor activities. Photophobia disappeared in 14 children in both atropine groups (3, 5 and 7 cases at about 5 months, 4 months and 1 month, respectively, in the 0.02% atropine group; 2, 6 and 6 cases at about 6 months, 4 months and 1 month, respectively, in the 0.01% atropine group). The symptoms of photophobia in the rest of the children were slightly alleviated but did not disappear. Average pupil diameter increases in children with photophobia were 0.90 mm and 0.86 mm in the 0.02% and 0.01% atropine groups, respectively. There was no significant difference in change in pupil diameter between the photophobia and no photophobia groups (p>0.05). Seven children in each of the atropine groups had mild near-vision blur for 2 to 4 weeks. But the near-vision blur disappeared gradually over time. One child was allergic to 0.01% atropine, resulting in symptoms of itch and eyelid swelling in the morning after 1 month of treatment. These symptoms disappeared after discontinuing the medication for 2 days. No children showed any other discomfort symptoms. In the control group, three children were photophobic in bright sunlight in the summer and one child experienced mild near-vision blur during the first week after changing to new glasses.
Discussion
In this double-blind and randomised controlled trial study, we found that low-concentration atropine drops, 0.02% and 0.01%, reduced myopia progression over a 12-month period, as measured by SER and AL, when compared with a control group. However, the effect was concentration dependent. Other consequences of treatment, such as change in pupil diameter and accommodative amplitude and reporting of discomfort symptoms, were similar between the two concentrations.
Atropine is a non-selective antagonist of muscarinic acetylcholine receptors. High concentrations of atropine block all receptor subtypes (M1, M2, M3, M4 and M5),21 22 but Loughman and Flitcroft23 thought that 0.01% atropine had minimal impact on pupil diameter and accommodative amplitude (M3 receptor), while retaining most of its beneficial effects on myopia progression (M1 and M4 receptors).20 Atropine has a dose-related response on the magnitude of myopia progression and side effects have been consistently reported at high doses (0.5% to 1.0%), but less consistently reported in moderate (0.01% to 0.5%) and low concentrations (0.01%). There is limited consensus on whether there is any difference in the efficacy and side effects of different concentrations of low-dose atropine.4 7 19 According to the current reports, the atropine concentrations (0.05%, 0.025% and 0.01%) that Yam et al7 used in their prospective, randomised, double-blind controlled study were similar to our study. Their subjects were children 4 to 12 years old (average about 8.4 years old) with myopia greater than −1.00D (average about −3.75D) and were followed up 1 year. They also found a concentration-dependent response on myopia progression in the three doses of atropine. Moreover, 0.05% atropine had the best myopia progression effect; 0.025% was the second and 0.01% had the least effect. In a 1-year study of Korean myopic children,19 AL elongation was 0.44±0.32 mm, 0.30±0.24 mm and 0.23±0.25 mm, respectively, for atropine concentrations of 0.01%, 0.025% and 0.05% atropine, with significant differences between groups. Conversely, Chia et al4 5 compared the safety and efficiency of 0.5%, 0.1% and 0.01% dose atropine in myopic children and found that there was a significant difference in myopia progression between the 0.5% atropine and 0.01% and 0.1% atropine, but there was no significant difference between the 0.01% and 0.1% groups after 1 and 2 years of follow-up. Meanwhile, they found that AL change at 1 and 2 years were all larger in the 0.01% atropine than in the 0.1% and 0.5% atropine, but there was no statistically significant difference between 0.1% and 0.5% atropine. These contrasting results might be due to the differences in the subject’s age, baseline SER and AL. For example, myopia progression appeared faster in a younger cohort in a previous study conducted in Hong Kong study.7
Pupil diameter increase and accommodative amplitude reduction count among the most important side effects when using muscarinic antagonists as an option for myopia progression.4 7 18–20 24 Our study found that 0.01% and 0.02% atropine had minimal and similar impact on pupil diameter and accommodative amplitude after 12 months of treatment. In previous studies using similar atropine concentrations to this study, Moon and Shin19 found that there was no difference in the pupil diameter increase, accommodative amplitude reduction, the frequency of near vision difficulties and photophobia after using 0.01%, 0.025% and 0.05% atropine for 1 year. Cooper et al20 compared the pupil diameter increase and accommodative amplitude reduction after using 0.01%, 0.02% or 0.05% atropine for 1 week. They reported a similar conclusion that 0.01% and 0.02% atropine had the same clinical effects on accommodative amplitude reduction and pupil diameter dilation. Kaymak et al24 observed the 1 day’s effects of very low-dose atropine (0.01%, 0.005% and 0.001%) on pupil diameter and accommodative amplitude in young adult. Clinically significant effects, on pupil diameter increase and accommodative amplitude reduction, were found for the 0.01% and 0.005% group. The magnitude of pupil diameter and accommodative amplitude effects were smaller at 0.005% than 0.01%, but 0.001% had minuscule effects on pupil diameter. Moon and Shin19 compared the side effects of 0.01%, 0.025% and 0.05% atropine for 1 year. They reported that 0.01% atropine had less change on accommodative amplitude and pupil diameter compared with 0.025% and 0.05% atropine, but there was no difference in the vision-related quality of life among all groups. These discrepancies could be explained by several factors. First, the atropine concentrations used were different (from 0.001%, 0.005%, 0.01%, 0.02%, 0.025% to 0.05%) in different studies. Second, changes in pupil diameter and accommodative amplitude varied with the age of the subjects. Accommodative amplitude decreased and pupil diameter increased more in older children than in younger children after the administration of low concentrations of atropine.23 The younger age at baseline of the subjects enrolled in our study may explain the smaller change in pupil diameter and accommodative amplitude experienced than the study reported by Loughman and Flitcroft.23 Third, atropine efficacy varies with race related to melanin levels within the iris.20 Iris melanin content can sequester anticholinergic compounds.25 A brown iris has two to four times more ocular melanin than an eye with a blue iris.26 Consequently, lighter irides would expect a greater pupil size and accommodation change than darker irides following use of the same atropine dosage.23
The most common ocular symptoms due to the use of low-dose atropine were photophobia and near-vision blur in this research, corroborating previous reports.4 7 18–20 24 In our study, we found that 23% and 33% children were photophobic in bright sunlight, and 4.9% and 5.1% children had mild near-vision blur for 2 to 4 weeks in the 0.01% and 0.02% atropine groups, respectively. Photophobia is presumably associated with reduced pupillary responsiveness and increased pupil diameter.23 Different studies have found different proportions of photophobia.4 7 20 In general, there is a higher proportion in the early stage after treatment. Cooper et al20 found that photophobia showed individual differences and was unrelated with age, sex, the degree of myopia and other parameters. Chia et al4 and Yam et al7 reported that pupil diameter was stable after treatment for 2 weeks. We also found that pupil diameters were unchanged after 4 months of treatment. Therefore, the finding that photophobia of some children disappeared with prolonged medication time may be related to drug tolerance and compensation, but not pupil miosis over time. Near-vision blur of some children may be related to decreased accommodative amplitude.20 The reason of a decline in accommodative amplitude may be due to the side effects of atropine itself and the dilated pupil diameter associated with the use of atropine. Dilated pupil diameter would decrease the depth of field and then decrease accommodative amplitude.27 According to the empirical formula of depth of field28: depth of field=±(0.75×pupil diameter−1+0.08). The influence of pupil diameter changes before and after 0.01% or 0.02% atropine on the depth of field was about 0.013D. By calculation, the decline in accommodative amplitude related to dilated pupil diameter was negligible compared with the total accommodative amplitude decline after atropine use. Consequently, the decline in accommodative amplitude was mainly related to atropine use.
The study was designed as a randomised controlled trial; however, advice from our human ethics committee mandated that at the randomisation visit, subjects were to be offered either atropine or no atropine and double-blinded randomisation to be carried out only for the two active arms of the study. We have shown that the control (no atropine) group was similar to the test arms in demographic and clinical parameters and subjects were recruited using identical inclusion criteria, contemporaneously and from the same population as the test arms. Although there were no baseline differences in factors that were measured, bias due to factors that were not measured, environmental factors such as near work time and outdoor activity10 11 cannot be excluded, although randomisation of the active treatment groups would be expected to minimise the impact of such factors. The pupil responsiveness was also not measured in the study. It may be associated with photophobia23 and should be considered in future atropine trials to confirm the present findings.
In conclusion, our preliminary findings showed that 0.02% atropine eye drops had a better effect on myopia progression than 0.01% atropine, but 0.01% and 0.02% atropine showed similar effects on pupil diameter, accommodative amplitude and symptoms of discomfort after 12 months of treatment. This study provided useful guidance and experience for the clinical use of low-concentration atropine to control the progression of myopia in children in Central Mainland China.
References
Footnotes
Contributors Study concept and design: AF, FS, YL. Acquisition, analysis or interpretation of data: AF, LW, WW, BZ, NJ, YL. Revised paper for important intellectual content and final approval of the version submitted for publication: AF, FS, KW, YL. Study supervision: YL.
Funding The study was funded by Medical Science and Technology Research Project of Henan Health Commission (201602073); Key R&D and Promotion Project of Henan Science and Technology Department (201801591); Key Scientific Research Project of Universities of Henan Education Department (19A320066).
Competing interests None declared.
Patient consent for publication Parental/guardian consent obtained.
Ethics approval This study was approved by the human ethics committee of the First Affiliated Hospital of Zhengzhou University (registration no. 2016-35).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available.