Article Text

Abstract
AIMS/BACKGROUND Recurrent erosion syndrome encompasses a group of mixed aetiologies for which there are a number of methods of management which may influence the course of the disease.
METHODS The outcomes of a cohort of patients initially treated with topical lubricants were studied. 117 consecutive patients presenting over 1 year with a history of recurrent erosions were enrolled, baseline characteristics were documented, and treatment with lubricants was initiated. Patients were surveyed 4 years later inquiring about symptoms and treatments required.
RESULTS A total of 94 (80%) of the initial cohort were contacted. The mean age was 44 years and the sex distribution was 44 males to 50 females. The mean period of follow up was 48 months. 55 (59%) were still symptomatic with attacks occurring at a median frequency of 60 days. 13 patients (24%) complained of an episode at least every week and 28 patients (51%) suffered at least every month. The median pain score (analogue scale of 1–10) was 2.5. Seventy five per cent (n=21) of patients with epithelial basement membrane dystrophy (EBMD) were symptomatic compared with those with a traumatic aetiology among whom 46% (n=28) were symptomatic. This difference was significant (p=0.02). Those with EBMD were more likely to be continuing to use topical lubricants than the trauma group.
CONCLUSION Patients with a traumatic aetiology are less likely to suffer chronic recurrent erosion syndrome than those with EBMD.
- recurrent erosion syndrome
- aetiology
- chronicity
Statistics from Altmetric.com
Recurrent erosion syndrome is a common condition that usually arises as a result of anterior stromal dystrophies, typically epithelial basement membrane dystrophy, or following trauma to the corneal surface. Rarely, cases may occur spontaneously without any obvious predisposing factor.
Symptoms of watering, redness, and photophobia typically occur on waking and may be associated with rapid eye movement sleep.
Two main forms of erosion have been characterised. In the microform condition there is a small epithelial break compared with the macroform condition where the break is larger with a surrounding loosely adherent epithelium. Typically, the microform condition occurs with spontaneous erosions associated with epithelial basement membrane dystrophy (EBMD), whereas macroform erosions are associated with a traumatic aetiology.1
The frequency of recurrence is variable ranging from a minor recurrence every morning to a major recurrence separated by several months. Recurrences typically last from 1 to 4 hours in the microform condition and 1 to 21 days in the macroform condition.1 The ultrastructural changes which reduce the adhesion of the epithelium include a deficient epithelial basement membrane, the absence and abnormality of hemidesmosomes, and the loss of anchoring fibrils.1-3
There is a plethora of treatments available for this condition which reflects their rather variable success rate. Simple conservative measures such as padding with bland lubricating ointment followed by the regular use of ointment at night have proved to be effective.4 5 More invasive treatments such as superficial keratectomy,6 anterior stromal puncture,7 or Nd:YAG8 and excimer laser therapy9-11 have been used. To date there are no randomised controlled trials comparing the various therapeutic techniques although there are numerous papers reporting the results of individual techniques.
In 1994 Hykin and others5 reported the results of a study where 117 consecutive patients with recurrent erosion syndrome were recruited. Patients with EBMD, those with focal epithelial abnormalities, and those with a normal corneal appearance were included in the study. Patients were further subdivided into those with a previous history of trauma and those in whom the presentation was acute or chronic. Patients with recurrent erosion syndrome caused by other corneal dystrophies were excluded. Patients with acute symptoms and an epithelial defect (n = 82) were initially treated with chloramphenicol ointment, padding, and cycloplegia. Following success with this treatment these, and those patients with chronic symptoms (n = 35), were randomised to receive a prophylactic regimen of either hypertonic saline ointment or simple ointment at night for 6 weeks. There was no observed difference in efficacy between the two regimens in preventing further attacks with 95% of patients being deemed as treatment successes. Successes included patients totally devoid of symptoms (45%) and those (50%) among whom some symptoms were experienced but whose symptoms were insufficient to interfere with their daily routine.
Following the completion of the study it became clear that many of these patients were sufficiently troubled by symptoms to require ongoing treatment or advice.
We aimed to review this well documented group of patients and to reinvestigate their symptomatology to establish the natural history.
Patients and methods
The original cohort of 117 patients were contacted either by a telephoned or mailed questionnaire. Specific questions were asked regarding symptoms which were attributed to recurrent erosion syndrome, the timing of those symptoms, and their frequency. Patients were asked to attribute an average pain score to symptoms using an analogue scale (range 1–10). Inquiry was made as to whether they were taking any ongoing treatments or whether they had sought further management advice, also as to whether any further surgical treatments had been used since the last review.
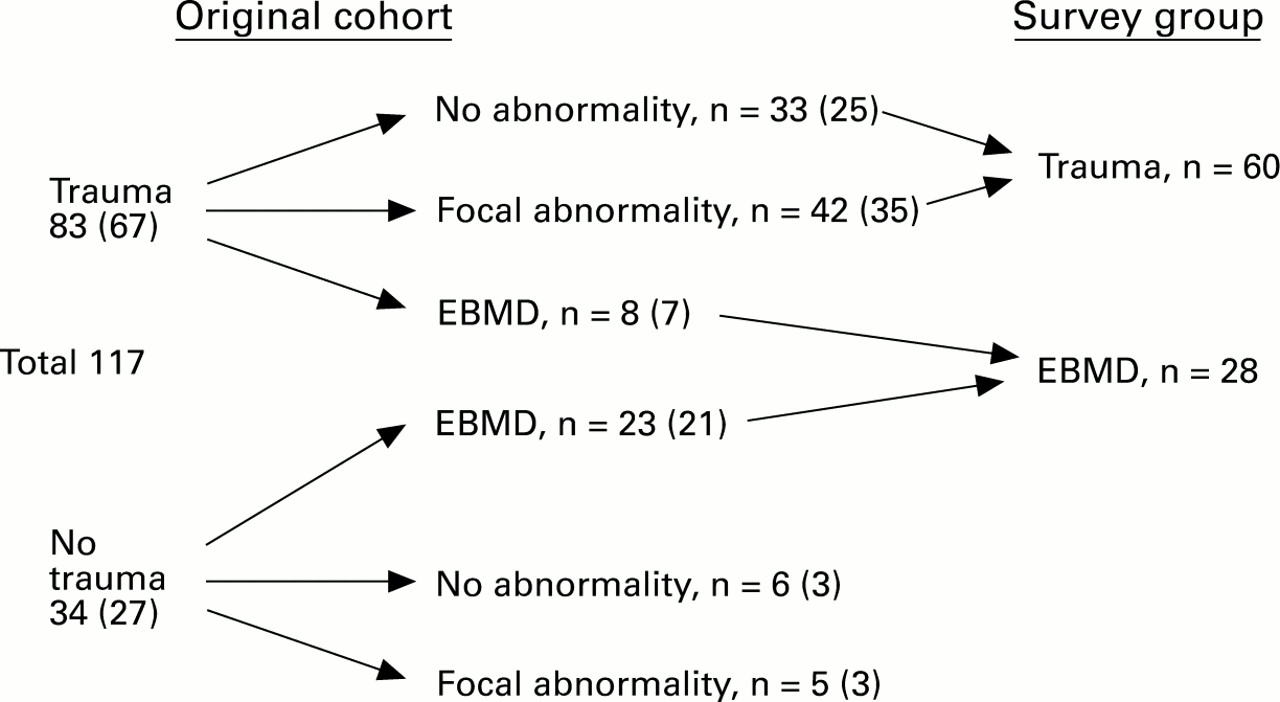
In order to simplify statistical analysis the subgroups in Hykinet al’s original clinical classification were stratified (Fig 1). Patients classified as EBMD with or without a history of trauma were stratified to a group labelled EBMD (n = 28). Patients classified as focal epithelial abnormality or no abnormality with a history of trauma were labelled as the trauma group (n = 60). This left six patients without classification under the new system. Placement of these six patients into either of the stratified groups did not alter the statistical results which were obtained using the χ2test. This number was considered to be sufficiently low to be ignored when statistically comparing the two groups.

The numbers of patients in Hykin’s original classification. The numbers contacted for this survey are shown in parentheses. The new survey group classification is also shown. EBMD = epithelial basement membrane dystrophy.
Results
Ninety four (80%) of the original cohort of patients were contacted; 44 were male and 50 were female. The mean age of all patients was 43.8 years (range 18–70 years). The mean follow up period was 48.2 months (4 years), range 39–69 months.
Fifty five patients (59%) were still symptomatic. Patients were deemed as symptomatic when it had been established that they were suffering from symptoms which they attributed to recurrent erosion syndrome. Fifty of the symptomatic patients (91%) complained of symptoms occurring upon waking in the mornings.
Compared with the trauma group the EBMD group were significantly more likely to be symptomatic ( p=0.02) but no more likely to require treatment (χ2 p = NS) (Table 1).
Percentages of each group who were symptomatic and the percentages of symptomatic patients who were on treatment
Overall, among patients who were symptomatic 55% (27/49) were taking some form of treatment which included topical drops or ointment. There was no difference in the types of treatment (lubricating drops or ointment) taken by the two groups.
Patients were most likely to self medicate (18/27, 67%); however, 26% (7/27) sought treatment from their general practitioner and 7% (2/27) required ophthalmic review.
The average frequency of attacks was assessed for each patient (Fig 2). These frequencies were those quoted as being the “average frequency” as perceived by the patient. The median frequency of the attacks was every 60 days; however, 24% (13/55) of symptomatic patients suffered with an attack at least every week and 51% (28/55) of the symptomatic patients suffered an attack at least every month. There was no difference in the frequency of attacks between the two aetiological groups.
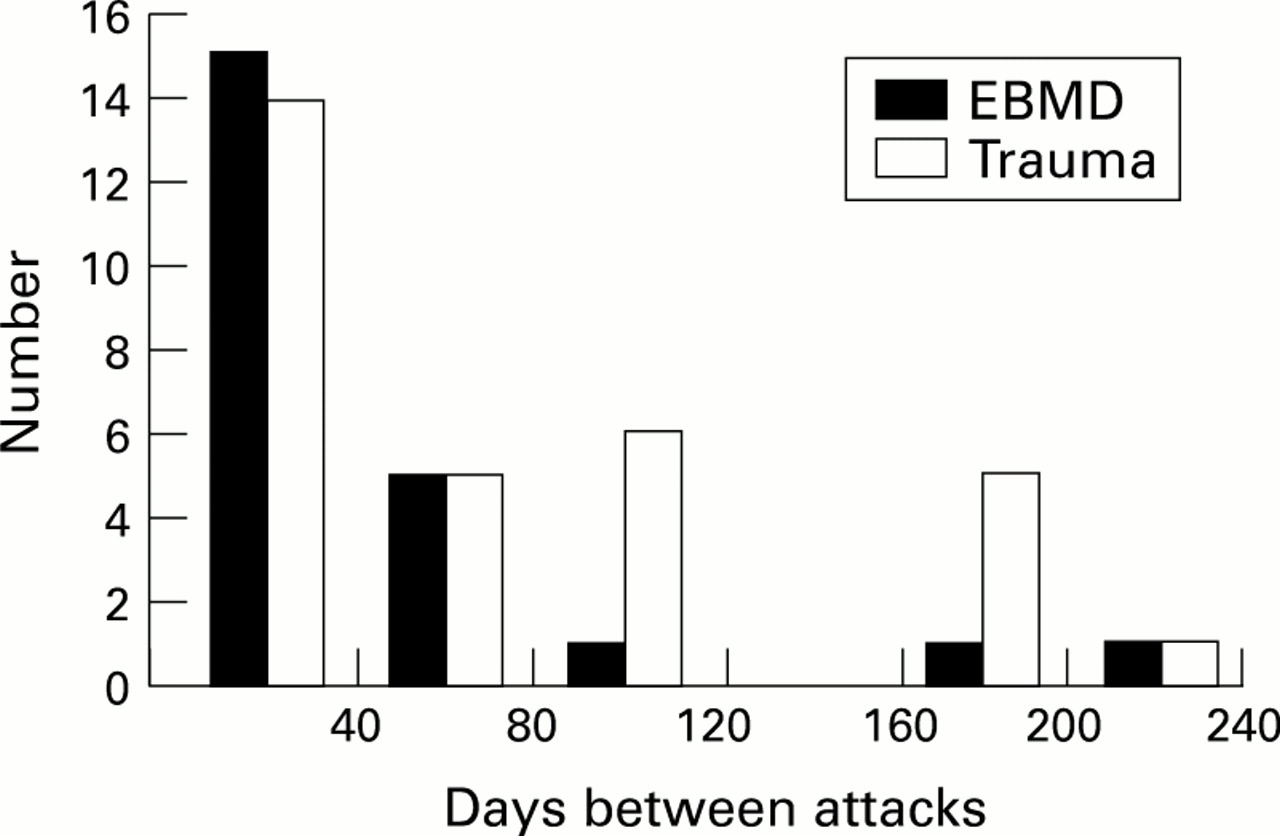
The frequency (perceived not recorded) of attacks for the EBMD and trauma groups. There was no statistical difference in the frequencies between the two groups.
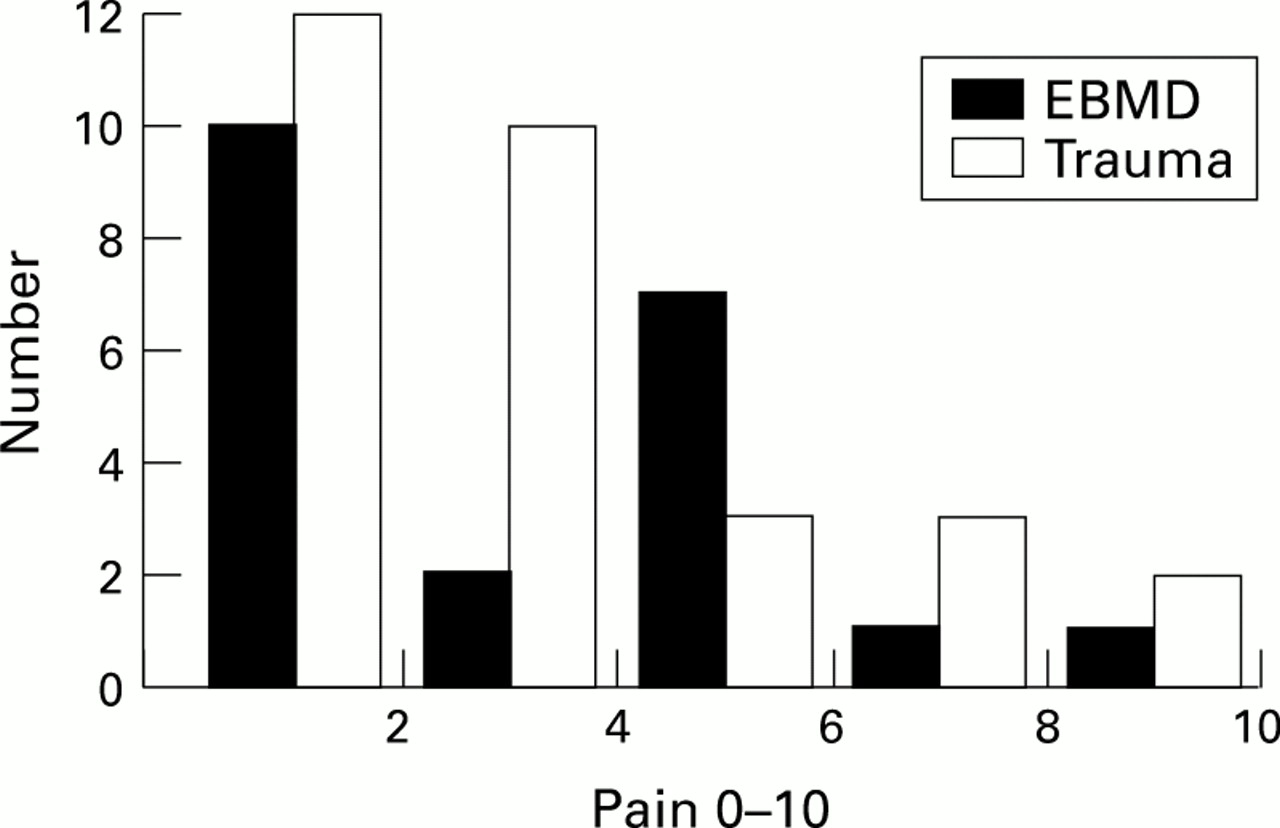
The median pain score (Fig 3) was 2.5 (range 0–10), with 56% (n=31) of patients with pain scores of 3 or less. There was no difference in the pain scores between the two groups.

{kind=link}
{kind=link}
{kind=link}
Pain scores (analogue scale 0–10) for the two groups. There was no statistical difference in the scores between the two groups.
Discussion
A significant number of patients with recurrent erosion syndrome were still symptomatic 4 years from initial review; however, this was more common in the EBMD group. The study was limited by being a questionnaire. Patients may have attributed a symptom erroneously but the fact that 91% complained of symptoms on waking strongly supports the fact that these symptoms could be attributed to recurrent erosion syndrome. The EBMD group were more likely to require some form of treatment than the trauma group, although there was no observed difference in the frequency of attacks and pain scores between the two groups. The increased use of treatment among the EBMD group may have masked any true difference in the frequency and severity between the two groups.
Because this study looked at patients with established recurrent erosion syndrome it does not follow that 60% of patients presenting with their first erosions following trauma or with EBMD will be symptomatic at 4 years. In fact, Jackson12 estimated the incidence of recurrence to be 1:150 cases following traumatic erosion.
We were unable to establish the degree to which patients are troubled by their symptoms in this study. How many of these patients would benefit from a more aggressive intervention is unclear. Interestingly, 50% of patients in Hykin et al’s study were still complaining of symptoms following treatment with topical lubricants despite having been deemed as treatment successes, since their symptoms were “insufficient to interfere with their daily routine”.5 The fact that 55% of symptomatic patients were still taking topical treatment after 4 years would suggest that a more aggressive treatment for this group may be appropriate.
When considering the surgical treatments for recurrent erosion syndrome it is important to define the goals. Öhman et al 10 reported the results of excimer laser treatment in 76 patients refractory to other treatments. Twenty one (27%) were still symptomatic following the treatment. Similarly, Rubinfeld et al 13 noted that although 24/25 patients were cured with anterior stromal puncture “a few” had continued ocular awareness and “many” continued with their nightly ointment. Buxton and Constad14 also noted that following epithelial keratectomy 11/33 (33%) were still reporting symptoms.
Clearly, surgical treatments do not provide the definitive answer to this problem. If EBMD is truly a dystrophy and not a degeneration then, following excimer laser treatment or epithelial keratectomy, that same abnormal epithelial phenotype with its basement membrane will repopulate the corneal surface. Although these treatments may in fact improve adhesion of the newly generated epithelium to Bowman’s membrane or the corneal stroma the epithelium is still phenotypically abnormal. This may partially explain why patients with traumatic recurrent erosion syndrome are less symptomatic in the long term than those with EBMD.
Doubtless, surgical treatments can offer relief from symptoms in a substantial number of patients, but controlled studies comparing treatment modalities for the various aetiological subgroups are required. Great care will be needed to standardise the results in terms of patient symptomatology.