Article Text

Abstract
AIMS To determine the prevalence of polypoidal choroidopathy in consecutive patients presenting with large haemorrhagic and exudative neurosensory retinal and retinal pigment epithelial detachments (PEDs) of over 2 mm in diameter in the absence of drusen.
METHODS 40 patients were identified over a 5 month period of which 29 had haemorrhagic detachments, and 11 had purely exudative detachments. All had indocyanine green (ICG) angiography, and the presence was sought of large blood vessels in the choroid associated with localised dilated terminals that filled slowly and leaked ICG.
RESULTS In 34 cases (85%) there was an appearance consistent with previous descriptions of idiopathic polypoidal choroidal vasculopathy. Of the six without polypoidal lesions the disorder was attributed to choroidal neovascularisation in four, chorioretinitis in one, and a fibrovascular PED in one. Of those with polypoidal lesions 20 (65%) were female, the mean age was 65.4 years (range 44–88), and 25 (74%) were white, seven (20%) black, and two (6%) east Asian. Eight had a history of hypertension. Visual acuity varied from 6/6 to counting fingers in the involved eye (mean 6/24). Bilateral polypoidal choroidal lesions were demonstrated in 16 patients (47%). The predominant location for these lesions was the macular region in 23 patients (68%). Polypoidal vasculopathy was found in 16 patients (47%) who had a previous diagnosis of age related macular disease (AMD). No patients had evidence of intraocular inflammation.
CONCLUSIONS In a largely white patient population a high proportion of patients with haemorrhagic and exudative PEDs has evidence of polypoidal lesions on ICG angiography.
- polypoidal choroidopathy
- pigment epithelial detachment
- retinal haemorrhage
- choroidal neovascularisation
Statistics from Altmetric.com
- polypoidal choroidopathy
- pigment epithelial detachment
- retinal haemorrhage
- choroidal neovascularisation
In the past, haemorrhagic detachment of the retinal pigment epithelium (PED) has been considered a part of the spectrum of age related macular disease (AMD), occurring as a consequence of age changes at the level of Bruch's membrane. Several mechanisms have been invoked to explain the pathogenesis of a PED, including decreased hydraulic conductivity of Bruch's membrane, choroidal neovascularisation, and excessive exudation from the choroidal blood vessels.1-3
Polypoidal choroidal vasculopathy (PCV) as a cause of recurrent haemorrhagic and exudative PEDs and neurosensory retinal detachments was first described in 1982.4 In the past, a variety of terms such as “posterior uveal bleeding syndrome” and “multiple recurrent retinal pigment epithelial detachments in black women” have been used to designate this disorder.5 6 It has characteristic morphological features that distinguish it from other exudative maculopathies, which include aneurysmal structures at the termination of a network of dilated choroidal veins associated with recurrent haemorrhage and leakage (Fig 1).

Illustration of three common presentations of idiopathic polypoidal choroidal vasculopathy. Along the superotemporal arcade, there are characteristic dilated choroidal vessels with an overlying pigment epithelial detachment (PED) and subretinal haemorrhage. Near the optic nerve there is a network of dilated choroidal vessels with polypoidal terminations with an overlying PED and subhyaloid haemorrhage. Along the inferotemporal arcade there is a ring of exudates surrounding a serous PED and neurosensory retinal detachment (RD) which overlies the polypoidal elements.
The diagnosis of PCV is best made using indocyanine green (ICG) angiography because it permits visualisation of the choroidal vasculature following the initial transit of dye.7 The increasing availability of ICG angiography has permitted a better appreciation of the prevalence and clinical presentation of the disorder. The original descriptions of idiopathic polypoidal choroidal vasculopathy associated the disorder exclusively with 50–65 year old hypertensive black females.8 Additional reports have expanded this definition and shown that it occurs in other races, but still attribute a high proportion of disease to darkly pigmented races.9 The location of the distinctive polypoidal lesions seen on ICG angiography was described as peripapillary in early publications. However, recent reports have shown that the lesions can also be present in the macular and extramacular regions.10 11
Because the definition of PCV continues to expand, we conducted a prospective study to seek evidence of polypoidal choroidopathy in patients with haemorrhagic and exudative neurosensory retinal and pigment epithelial detachments in whom there was no evidence of age changes at the level of Bruch's membrane.
Materials and methods
We conducted a prospective analysis of consecutive patients identified with haemorrhagic and exudative PEDs over 2 mm in diameter during a 5 month period from August 1998, to the end of December 1998, who presented to the medical retina unit in a tertiary referral centre. A total of 40 patients were included in the study, of which 16 patients were seen as new referrals and 24 as return visits.
Our inclusion criteria were haemorrhagic or exudative retinal PED or neurosensory retinal detachment equal to or greater than 2 mm on ophthalmic examination. Patients with drusen in either eye, fluorescein angiographic evidence of classic choroidal neovascular membranes or tears of the retinal pigment epithelium were excluded as they were considered to have clear evidence of AMD as it is usually recognised in a white population. Patients with opacification of media that precluded a fundus examination or allergy to fluorescein dye were also excluded.
All patients underwent general ophthalmic examination including indirect ophthalmoscopy and slit lamp biomicroscopy followed by colour photography. Digital fluorescein and indocyanine green angiography were performed on all patients using a Topcon TRC 50X fundus camera (Topcon, Bracknell). Hard copy prints were made using a Kodak DS 8650PS Printer (Kodak, Hemel Hempstead). PCV was defined by the previously determined characteristics on ICG angiography of a branching network of wide diameter vessels terminating in multiple areas of aneurysmal swelling that were anterior to the choroidal vessels on stereoscopic examination.9 The diagnosis was made by two masked observers, and in the case of disagreement, a third served as arbitrator. The location of the polypoidal lesions was assigned to one of the following three locations based on ICG findings: peripapillary, macular, or extramacular. A peripapillary location was defined as within one disc diameter from the optic nerve. A macular lesion was that lying within the temporal retinal vascular arcades. An extramacular lesion was that lying outside the temporal retinal vascular arcades. In cases with polypoidal vascular complexes in multiple sites, the location was designated by the largest complex.
Medical disorders such as hypertension and diabetes were identified by previous diagnosis or by the use of appropriate systemic medications. Statistical analysis for descriptive statistics was performed usingspss statistical software (SPSS, Inc, Chicago, IL, USA). This study was approved by the Moorfields Eye Hospital ethics committee.
Results
Of the 40 patients included in the study, 29 had haemorrhagic PEDs, and 11 had exudative PEDs, each with or without neurosensory retinal detachments. On ICG angiography 34 of the 40 patients had evidence of polypoidal lesions consistent with PCV (Figs 2–6). Of the six patients without polypoidal lesions the clinical findings were attributed to either choroidal neovascular membrane, or a fibrovascular PED the origin of which was uncertain.
Of the 34 patients with PCV 12 (35%) were male and 22 (65%) female, and the mean age was 65.4 years (range 44–88), 25 (74%) were white, seven (20%) black, and two (6%) of east Asian origin. Eight patients had a history of hypertension and one had a history of diabetes (Fig2). Two patients were taking aspirin regularly, and none were on other anticoagulant therapy.

Right eye of a 68 year old black male with 6/36 vision. (A) Photograph showing a large area of subretinal haemorrhage with exudate and hyperpigmentary changes located superior to the superotemporal arcades. Along the superotemporal vessel there are two elevated subretinal lesions. (B) Fluorescein angiogram showing blockage of fluorescence by the subretinal blood and multiple areas of hyperfluorescence. (C) ICG angiogram showing a choroidal vascular network terminating in multiple polypoidal-like elements along the superior vessel which correspond to the subretinal lesions seen on the photograph.
Sixteen patients (47%) had bilateral polypoidal lesions with choroidal vascular complexes as seen on ICG angiography. In some cases there were no symptoms referable to the fellow involved eye, and in others visual loss had occurred previously. In one case there appeared to be choroidal neovascularisation (CNV) and polypoidal lesions in one eye, but the other had polypoidal lesions only (Fig 3). In another there was total exudative detachment in the other eye and a vision of no light perception that had occurred spontaneously. There was a strong suspicion that this was due to PCV although we could not confirm this. Of the 50 affected eyes visual acuity ranged from 6/6 to counting fingers (mean 6/24). A minority of patients had long lived serous detachments of the retina, and there was also evidence of hypertrophic subretinal tissue in some.

(A) Photograph of the left eye of a 75 year old black man with 6/18 vision showing a haemorrhagic PED with a nasal notch, scattered intraretinal haemorrhages, and old peripheral panretinal laser photocoagulation scars inferiorly. (B) Mid-phase fluorescein angiogram showing staining of the PED, hyperfluorescence in the area of the notch, blockage of fluorescence by the haemorrhage, and hyperfluorescent staining of the peripheral laser photocoagulation scars. (C) Early ICG angiogram showing two areas of a grape-like cluster of polyps in the peripapillary region in the area corresponding to the notch seen on fluorescein angiography.
The predominant location for these polypoidal lesions was the macular region in 23 patients (68%), peripapillary in six (18%), and extramacular in five (14%) (Figs 3 and 4). Many of the macular and peripapillary polypoidal lesions were located immediately adjacent to the PEDs (Fig 5). Previous or referring diagnoses of patients ranged from AMD in 17 (50%), idiopathic central serous chorioretinopathy (CSC) in six (18%), unknown in five (14%), macroaneurysm in two (6%), chorioretinitis in two (6%) and diabetes and PCV in one each, respectively. No patients had evidence of intraocular inflammation.
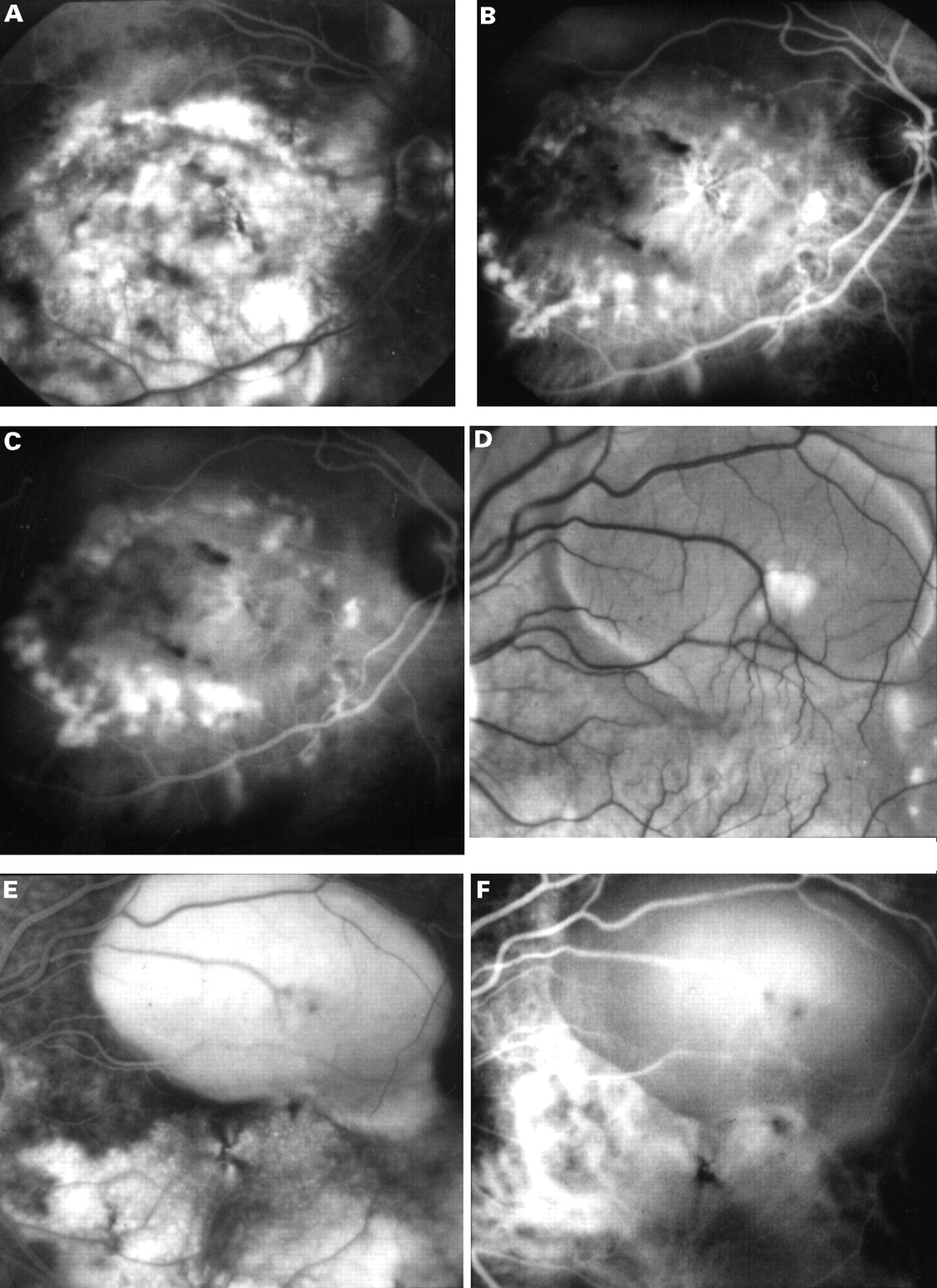
(A) A late fluorescein angiogram of the right eye of a 54 year old white man with counting fingers vision showing diffuse areas of hyperfluorescence between the temporal vascular arcades corresponding to a large serous elevation of the retina with subretinal fibrosis, hyperpigmentary changes, and subretinal and intraretinal haemorrhages. (B) Early ICG angiogram showing a ring of polyp-like aneurysmal dilatations of the choroidal vasculature in the macular region. In addition, there appears to be a choroidal neovascular complex centrally. (C) The mid-phase ICG showing staining of these polypoidal lesions. (D) In his left eye there was a pigment epithelial detachment. (E) Fluorescein angiography showed filling of the detachment and diffuse hyperfluorescence below and nasal to the lesion. (F) ICG angiography revealed a large diameter vessel complex at the same site with terminal dilatation of the vessels.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
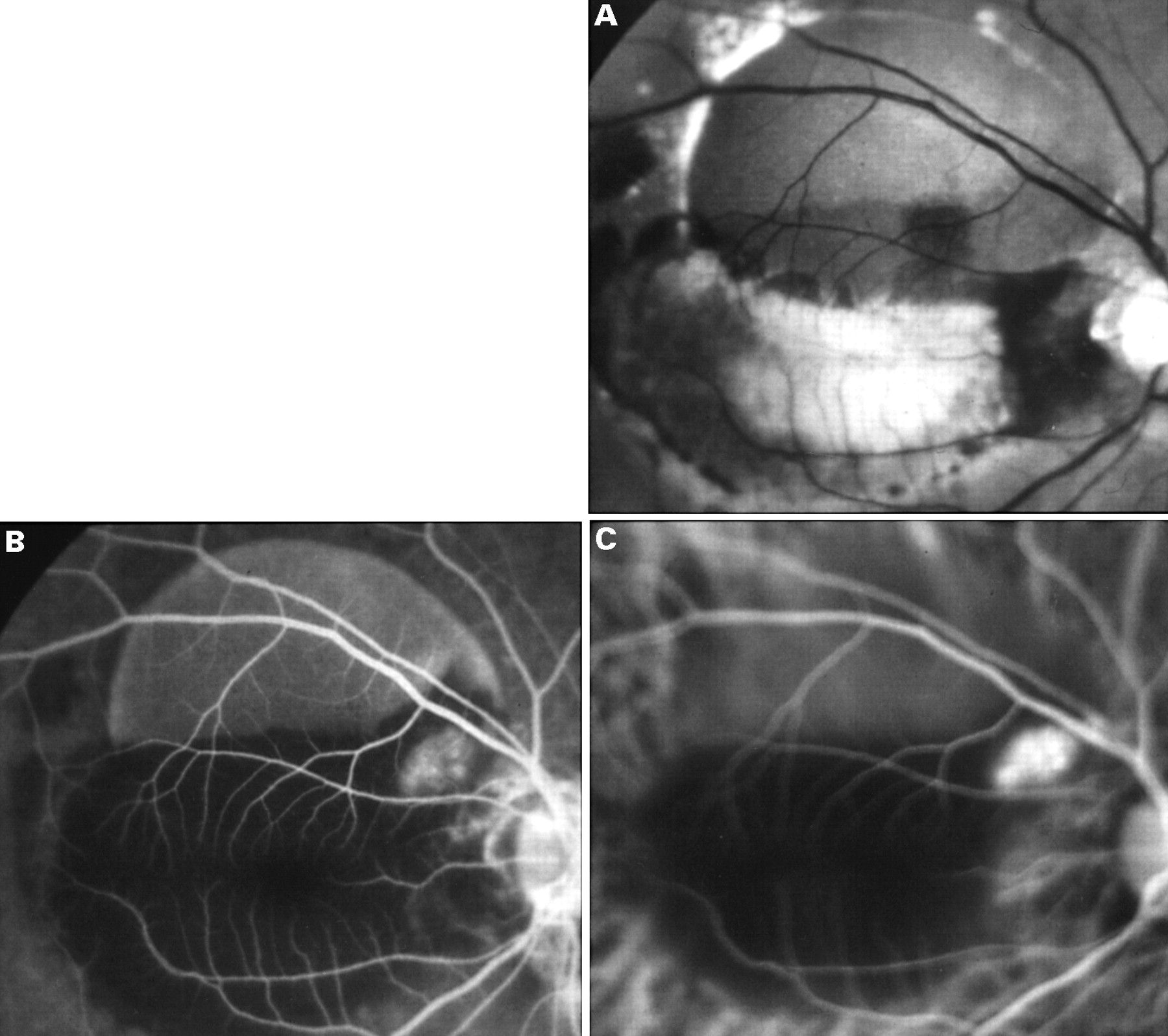
(A) The right eye of a 58 year old black male with 3/60 vision showing a large serous PED along the superotemporal arcade with surrounding subretinal haemorrhage and intraretinal exudate. (B) An early phase fluorescein angiogram showing filling of the PED, blockage of fluorescence by the subretinal exudate and haemorrhage, and a distinct hyperfluorescent lesion adjacent to the PED near the optic nerve head. (C) An early phase ICG angiogram showing a complex of polypoidal lesions in a “grape-like cluster” adjacent to the PED corresponding to the area of hyperfluorescence seen on the fluorescein angiogram.
Discussion
The definition of PCV has expanded over the past 10 years, and the diagnosis is no longer restricted to specific demographic attributes or to a specific retinal location.10-14 In a major review by Yannuzzi and colleagues white patients comprised 20% of all cases that had been previously reported, although the disorder is still considered to largely affect darkly pigmented races in higher proportion.9 By contrast, a majority of our patients with PCV were white, admittedly in a patient population that is largely white. Previously, the location of the polypoidal lesions had been thought to be limited to the peripapillary region, but Moorthy and colleagues described macular lesions in eight patients.10A single case of a peripheral PCV has also been described.11 The polypoidal complexes in our patients were predominantly macular in location, and few were extramacular implying that the diagnosis of PCV should not be limited to peripapillary disease.
In most other respects our findings are similar to those of previous authors. The mean age was similar to that found in previous studies, 65 years, but with an expanded age range including an 88 year old. The majority of our patients were women (65%). Unlike AMD, fibrovascular disciform scarring is reported as unusual in PCV, though some of our patients had hypertrophic subretinal scars.15 A greater degree of intraretinal exudate and subretinal haemorrhage is also characteristic of PCV.
Before 1994, the characterisation of PCV was based on clinical findings and fluorescein angiography. Later studies have shown that most cases cannot be recognised without the use of ICG angiography. As in previous studies, we found the ICG angiographic features of polypoidal lesions to be distinct from those of CNV.9 13 The prominent choroidal wide diameter vascular complexes ending in aneurysmal dilatation of PCV fill relatively late on ICG angiography and are associated with intense fluorescence late. The dilated choroidal veins sometimes obscured visualisation of the terminal polyp-like bulbs, and stereo-imaging was important in distinguishing the complex from the underlying dilated choroidal veins.
There have been references to the association of PCV with other ocular disorders such as idiopathic central serous chorioretinopathy (CSC), chorioretinitis, and retinal macroaneurysm.9 16 17 The exudative PEDs that occur in PCV are similar to those found in CSC, and five of our cases had a previous diagnosis of chronic CSC. There is as yet no evidence of a pathogenic relation between the two conditions, although in both there is leakage from the choroidal vessels on angiography.18 19 Ross and colleagues reported a correlation between retinal macroaneurysms and PCV in two hypertensive black women.17 They proposed a relation between the retinal vascular changes in retinal macroaneurysms and hypertensive retinopathy such as vascular remodelling, aneurysmal dilatation, and focal vascular constriction to the characteristic choroidal lesions in PCV. We found no evidence of a close association between PCV and systemic disorders such as hypertension in our study population which is in accord with most recent reports.
In a clinicopathological correlation in a case of PCV, MacCumber and associates found that the recurrent serosanguineous detachments of the RPE were secondary to CNV with extensive fibrovascular proliferation in the subretinal space and within Bruch's membrane.16 They observed some large choroidal veins but did not find choroidal localised dilatations of the choroidal vessels. It is possible that the neovascularisation was a secondary event rather than the precipitating disorder. Although there was no clinical evidence of inflammation in this patient, immunohistochemistry demonstrated both B and T lymphocytes in the choroid and fibrovascular tissue. There is no clearly established link between the inflammatory changes and the presence of choroidal vascular abnormalities in this patient. The histopathology still has not clearly been defined in cases that have a good clinical correlation.
PCV may represent a variant of AMD as is commonly recognised in a white population, or the two conditions might be quite distinct. In the earliest reports there was no proposed association between the characteristic lesions of PCV and AMD.5 6 As in our study, polypoidal lesions have been recognised in a white patient previously diagnosed as having exudative AMD.14 The features previously used to distinguish AMD from PCV included: white race, macular location, presence of drusen, frequent recurrence, rapid rate of progression, disciform scarring, and poor visual prognosis.12 13
It is evident that the pathogenesis of PCV is in doubt that is to some extent related to the lack of histopathological studies. They do not occur is eyes with pre-existing changes in Bruch's membrane. It appears to be a slow flow system. The lack of choroidal neovascularisation after photocoagulation17 suggests that the process is not associated with the neovascular drive characteristic of CNV. The overall visual prognosis of PCV is reported to be less predictable than that of AMD associated with CNV and PED in that spontaneous recovery has been reported in lesions in which recovery would not be expected in the context of AMD.20-22 The assumption that peripheral vision is not affected by AMD cannot be translated to PCV.
Whether or not genetic or environmental factors have a role in the pathogenesis of PCV as they do in AMD remains to be determined. Yannuzzi and associates suggested that in Asians PCV “may masquerade as neovascularised AMD”.9 The phenotype of macular disease with pigment epithelial detachments without drusen in middle age and older east Asians indicates that PCV is common in these communities.
Our recent experience suggests that PCV is much more common than we had appreciated. To some extent our failure to recognise this condition was based on preconceived ideas as to its phenotype and those at risk of having the disorder. We excluded from our survey patients with evidence of AMD, although it is unlikely that drusen protect against PCV. Thus, the condition may be more common than this study suggests. It is only with a full cross sectional study of those over 45 years of age with macular disease that the true prevalence of PCV will be identified. There is clearly good reason to make the diagnosis since it appears that the condition may respond well to laser photocoagulation.13 23 24 If the complexes are slow flow systems without neovascular drive, success in obliterating the lesions is likely to be high and recurrence low.