Article Text

Abstract
Objective To determine the efficacy and safety of azithromycin 1.5% eye drops in a paediatric population with purulent bacterial conjunctivitis.
Patients and methods This was a multicentre, international, randomised, investigator-masked study in 286 children with purulent discharge and bulbar conjunctival injection. Patients received either azithromycin 1.5% eye drops (twice daily for 3 days) or tobramycin 0.3% eye drops (every 2 h for 2 days, then four times daily for 5 days). Clinical signs were evaluated on day (D) 0, 3 and 7, and cultures on D0 and D7. The primary variable was the clinical cure (absence of bulbar conjunctival injection and discharge) on D3 in the worse eye for patients with positive cultures on D0.
Results 286 patients (mean age 3.2 years; range 1 day–17 years) were included; 203 had positive cultures on D0. Azithromycin was superior to tobramycin in clinical cure rate on D3 (47.1% vs 28.7%, p=0.013) and was non-inferior to tobramycin on D7 (89.2% vs 78.2%, respectively). Azithromycin treatment eradicated causative pathogens, including resistant species, with a similar resolution rate to tobramycin (89.8% vs 87.2%, respectively). These results were confirmed in a subgroup of patients younger than 24 months old.
Conclusions Azithromycin 1.5% eye drops provided a more rapid clinical cure than tobramycin 0.3% eye drops in the treatment of purulent bacterial conjunctivitis in children, with a more convenient twice-a-day dosing regimen.
- Child Health (paediatrics)
- Conjunctiva
- Infection
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Conjunctivitis is one of the most common eye infections in childhood and a common cause of paediatric primary care visits and ocular complaints in paediatric emergency departments 1–3. Bacterial infection accounts for up to 50% of all conjunctivitis cases in adults and as many as 70–80% of cases in children3.
Bacterial conjunctivitis is characterised by mucopurulent discharge and conjunctival hyperaemia4. It is an extremely contagious disease caused by one or more bacterial species and affects both sexes, all ages, ethnicities and countries. It can also cause epidemics among people in close quarters, including nursery, school and student populations5 ,6. Mild cases are generally considered to be self-limiting, resolving in 5–10 days. However, current consensus supports the use of topical antibiotics as they provide significantly better rates of early clinical cure and microbiological resolution compared with artificial tears7–10. Topical antibiotics are also known to reduce the rate of reinfection and prevent infection spread7.
There are only a few available options for the treatment of purulent bacterial conjunctivitis with topical antibiotics in children11 as most available topical antibiotics have been approved based on clinical studies performed only in adults. Although regulatory health authorities worldwide encourage paediatric clinical studies, the efficacy and safety of topical antibiotics are yet to be formally tested in this population. Thus, specific clinical data are still required for children with this indication.
In this study, azithromycin 1.5% ophthalmic solution, a topical antibiotic option recently approved in Europe for the treatment of bacterial conjunctivitis and trachomatous conjunctivitis12, was tested in children as young as a few days old. The objective of this study was to determine the efficacy and safety of azithromycin 1.5% eye drops and also its rapidity of action (from say [D] 3) in order to support its indication in children, notably in those younger than 2 years old. Secondary objectives included determination of infection bacteriological profiles and microbiological resolution rates.
Methods
Study design and patients
This multicentre, international, randomised, investigator-masked, parallel-group study was performed to compare the efficacy and safety of azithromycin 1.5% (Azyter, Laboratoires Théa, France) versus tobramycin 0.3% (Tobrex, Laboratoires Alcon, France) eye drops in paediatric patients. The study was conducted between December 2008 and February 2011 in 21 investigational centres across eight countries (France, Germany, Italy, Poland, Portugal, Romania, Algeria and Tunisia).
Eligible patients were children (from 1 day to 18 years old) with purulent bacterial conjunctivitis, defined by mild to severe bulbar conjunctival injection and purulent discharge in at least one eye. Patients were excluded if they were premature newborns or had associated ocular pathologies. Systemic or ocular antibiotics, anti-inflammatory or immunosuppressive treatments were not authorised for use during the study.
The study was conducted in accordance with Good Clinical Practice, the Declaration of Helsinki and local regulations. Ethics committee approvals were obtained in each country prior to enrolling any patient. Written informed consent was obtained from parents/guardians. The trial was registered at http://clinicaltrials.gov under the reference number NCT01155999.
Treatment administration
On D0, eligible patients were randomly allocated (1:1 ratio) to one of the two investigator-masked study treatments. The randomisation was stratified by age group (<4, 4–12 and 12–18 years). Patients received either azithromycin 1.5% eye drops, one drop twice-daily (morning and evening) from D0 to D2, or tobramycin 0.3% eye drops, one to two drops every 2 h on D0–1, up to 8 times/day, then one drop 4 times/day on D2–6.
Study assessments and outcomes
All patients were to attend three visits (D0, D3 and D7). A ‘first ophthalmologist investigator’ who was masked to the treatment performed the ophthalmologic examination, while a second investigator was responsible for dispensing medications and assessing tolerance and safety.
Clinical efficacy assessments
Cardinal clinical signs of bacterial conjunctivitis (bulbar injection and purulent discharge) were assessed for each eye under slit lamp and scored using a four-point scale, as described previously9 ,13–15. The primary efficacy variable was clinical cure as defined by the absence of bulbar conjunctival injection and purulent discharge in the worse eye on D3 in the microbiologically positive full analysis set (MFAS; patients with positive bacterial cultures on D0). Secondary efficacy variables included clinical cure on D7, other ocular signs (folliculo-papillary reaction of palpebral conjunctiva, eyelid erythema, eyelid swelling) and symptoms of bacterial conjunctivitis scored on a four-point ordinal scale (0=absent; 1=mild; 2=moderate; 3=severe; preverbal patients were not assessed for symptom scores).
Microbiological assessments
A conjunctival swabbing was taken from each infected eye on D0 and D7. Bacterial specimens were analysed by a local laboratory using standard validated methods. The bacteriological status was confirmed by an independent central review using the modified Cagle's classification16. A bacteriological sample was considered positive if bacteria isolated after culture were above the pathogenic thresholds following Cagle's microbiological criteria. Microbiological resolution (ie, absence of bacteria or their reduction below the pathogenic threshold) was assessed on D7.
Safety assessments
The safety analysis was based on the evaluation of adverse events (AEs), symptoms related to study medication instillation (ie, burning/stinging/itching, stickiness, foreign body sensation and blurred vision), ocular signs at slit lamp examination, visual acuity and treatment tolerability by the investigator and patient or parent/guardian. For preverbal children, unusual discomfort upon instillation was assessed by parent/guardian. If an exacerbated reaction was noted by the parent/guardian upon instillation of the study medication to his/her child, the symptoms of itching/burning/stinging, stickiness, foreign body sensation and blurred vision were recorded.
Statistics
Based on the superiority hypothesis used previously17, it was estimated that 111 patients with positive cultures on D0 were required in each treatment group in order to have a 80% probability of showing a difference of 20% in the clinical resolution rate between azithromycin 1.5% and tobramycin 0.3% (48% vs 28%) with α of 0.05 (two-sided 95% CI) on D3.
The primary efficacy variable was analysed in the MFAS using the exact Cochran–Mantel–Haenszel (CMH) test stratified by age group. Moreover, azithromycin 1.5% was considered non-inferior to tobramycin 0.3% if the lower bound of the exact 95% CI of the treatment difference (azithromycin–tobramycin) was ≥−10%18. A CMH test was also used for other between-group comparisons. All comparisons were performed two-sided at the 5% α level. For the supplementary tests in the age subgroup 0–2 years, a Bonferroni correction was applied, and resulting p values were interpreted at a significance level of 1.25%. Missing data were handled by using the last available assessment. For confirmatory purposes, analyses were performed on the microbiologically positive per protocol set (MPPS) and for the contralateral infected eye. Tolerance and safety were evaluated for the safety population (all patients who used study medication).
Results
Patient demographics and baseline characteristics
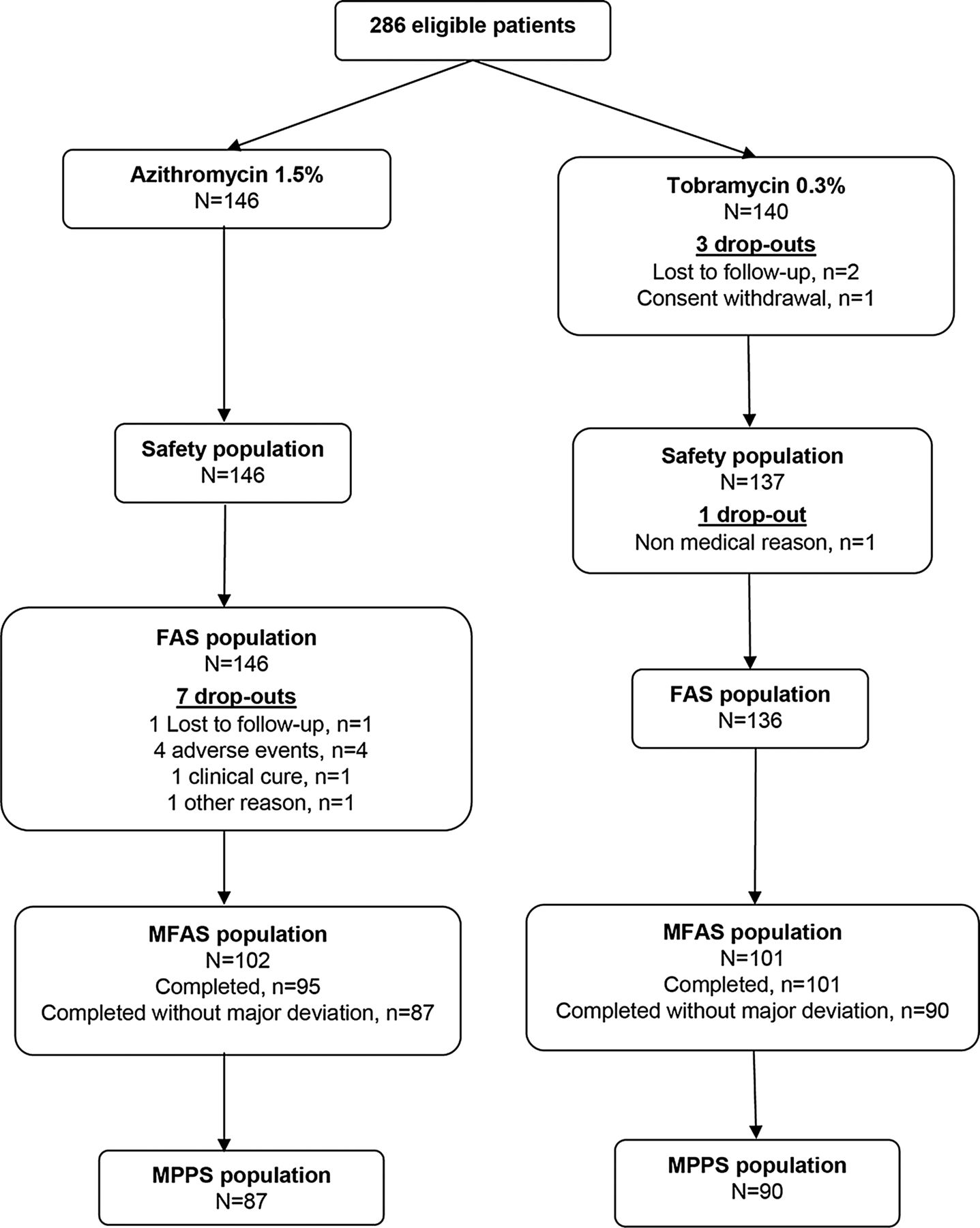
A total of 286 eligible patients were randomised (figure 1). Of these patients, 203 (71.0%) with baseline bacterial cultures at/above the pathogenic threshold in at least one eye were included in the MFAS. Seven patients on azithromycin (4.8%) and four patients on tobramycin (2.9%) withdrew from the study. In the MFAS, 8 azithromycin-treated patients and 11 tobramycin-treated patients had major protocol deviations and were excluded from the MPPS.
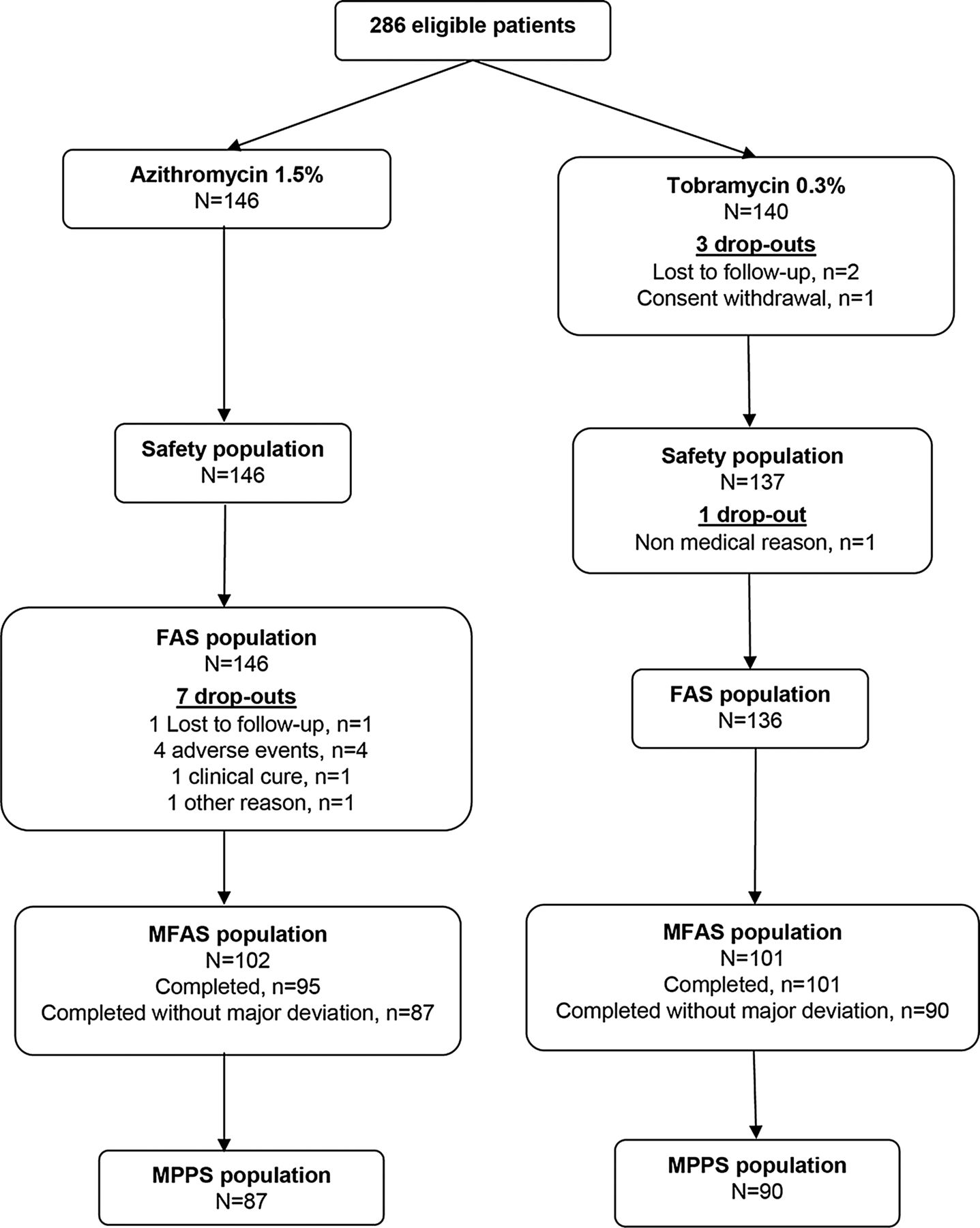
Study flow chart.
There was no notable between-group difference in the MFAS regarding baseline characteristics (table 1). The mean age was 3.0±3.4 years, and 55.2% of patients were younger than 24 months old. Overall, 66.0% of patients had moderate to severe bulbar conjunctival injection in the worse eye at baseline, and 87.2% had moderate to severe purulent discharge. The severity of both these cardinal clinical signs was not significantly different between treatment groups at baseline (p=0.559 and 0.729, respectively). Folliculo-papillary reaction was present in 52.2%, eyelid erythema in 41.9% and eyelid swelling in 38.4% of patients, without notable between-group difference in severity (p=0.561, 0.673 and 0.548, respectively).
Patients’ characteristics at baseline (MFAS)
Clinical efficacy
On D3, the clinical cure rate for the worse eye was significantly higher in the azithromycin group compared with the tobramycin group for patients in the MFAS (47.1% vs 28.7%, respectively; p=0.013) (table 2). On D7, there was no statistically significant difference in clinical cure rates between treatment groups (89.2% vs 78.2%, respectively; p=0.077), and non-inferiority of azithromycin to tobramycin was demonstrated. Similar rates were found for the contralateral eye and in the MPPS (data not shown).
Clinical cure rate in the worse eye (MFAS)
Improvements of other ocular signs (folliculo-papillary reaction, eyelid erythema, eyelid swelling) were also noted on D3 and D7, but were not significantly different between groups (D3: p=0.067, 0.662 and 0.498, respectively; D7: p=0.172, 0.421 and 0.165, respectively).
Bacterial resolution
The most frequent causative microbes isolated from patients at inclusion were Haemophilus (31.5%), Staphylococcus aureus (17.7%), Streptococcus pneumonia (14.8%), coagulase-negative Staphylococcus (12.8%) and Staphylococcus epidermidis (11.3%) (table 3). Overall, the bacteriological resolution rate in the worse eye on D7 was similar in both groups, with no notable difference between treatments (p=0.679). A higher resolution rate was noted for S aureus in patients treated with azithromycin (93.8%) compared with tobramycin (75.0%); however, this was not statistically significant (p=0.252).
Bacteriological resolution (for Cagle-regrouped microbes and global) in the worse eye on day 7 (MFAS)
Clinical cure and bacteriological resolution in patients younger than 24 months
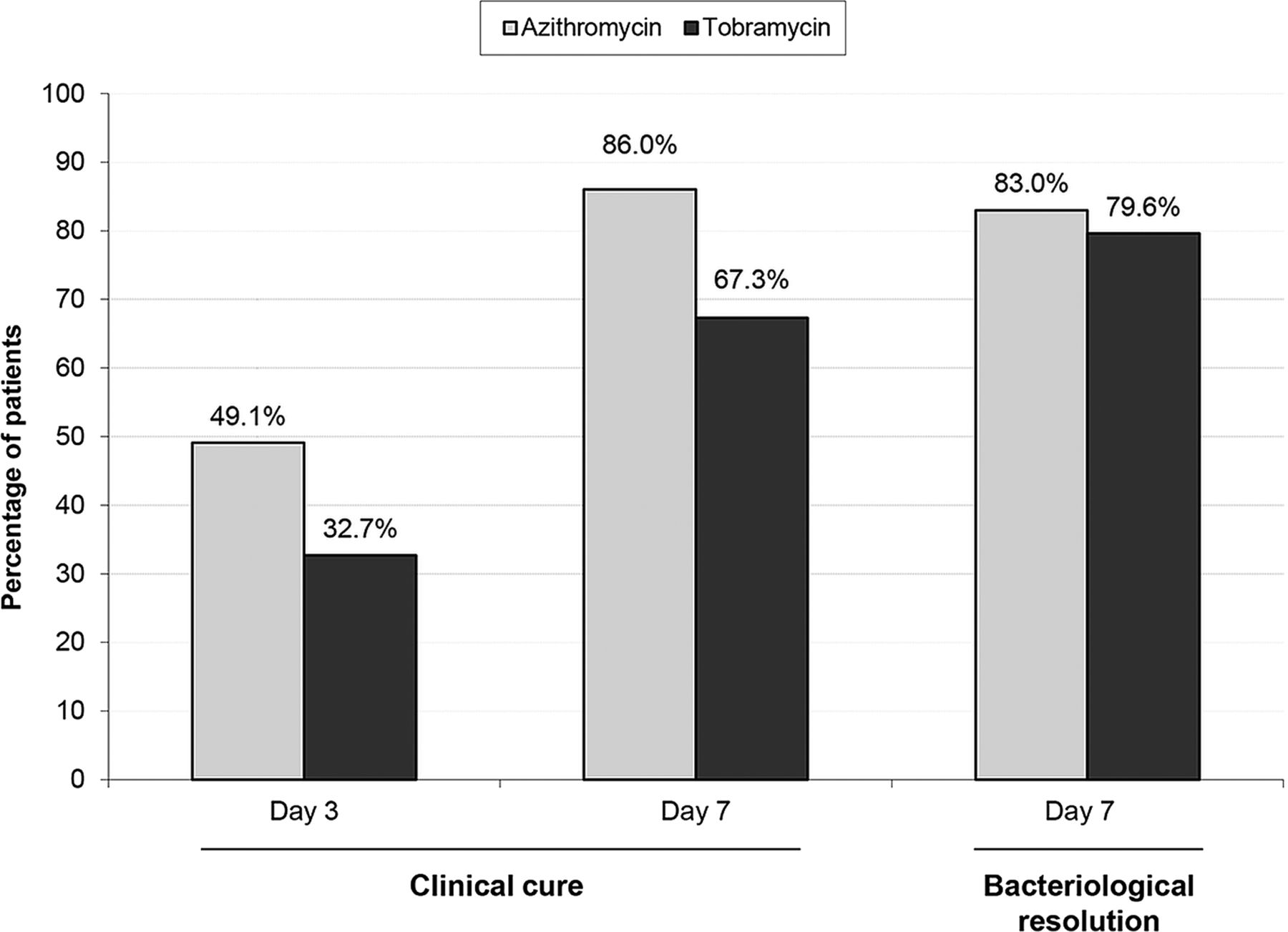
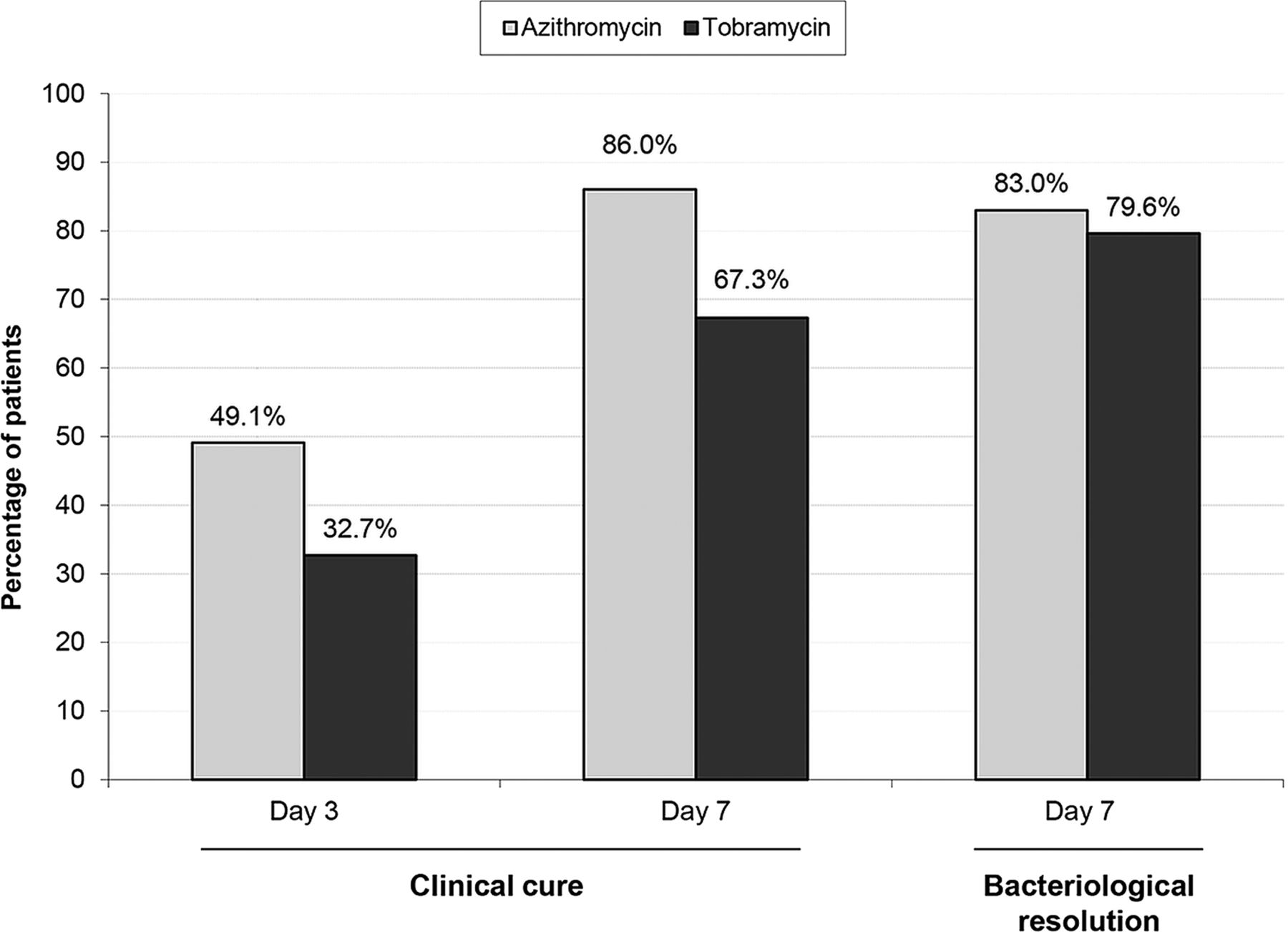
Additional analyses performed in the subgroup of patients younger than 24 months old showed similar clinical cure and bacteriological resolution rates compared with the MFAS (figure 2). Clinical cure was achieved for a higher percentage of azithromycin-treated patients compared with tobramycin-treated patients on D3 (49.1% vs 32.7%, respectively; p=0.079) and D7 (86.0% vs 67.3%, respectively; p=0.020). Bacteriological resolution rates on D7 were similar in both groups (p=0.672).
{kind=link}
{kind=link}
Clinical cure and bacteriological resolution in the worse eye in patients aged <24 months (microbiologically positive full analysis set, N=112).
Safety
In all, 283 children were evaluable for safety (figure 1). Both treatments were well tolerated in all age categories, with no serious ocular AEs reported. One case of hypersensitivity (severe right hemifacial erythema) was reported in a 6-month-old azithromycin treated-patient. Ocular AEs considered by the investigator as related to the study drug were reported in four patients (2.7%) treated with azithromycin and one patient (0.7%; p=0.209) treated with tobramycin. These included erythema of the eyelid, eyelid oedema and ocular hyperaemia. All treatment-related ocular AEs were mild, except for one case of severe ocular hyperaemia in the azithromycin group.
Itching/burning/stinging was the most common instillation-related ocular symptom reported on D3 in both treatment groups and was rated as ‘disturbing’ or ‘very disturbing’ for 7.6% of patients on azithromycin and 0.8% of patients on tobramycin (p=0.003). Neither corneal inflammation nor active inflammation of the anterior chamber was noted for any patient on slit lamp examination. Clinically significant superficial punctate keratitis was found in one azithromycin-treated patient (>4 years) on D3, but this had resolved by D7.
Overall, patient-/guardian-rated and investigator-rated tolerability was good. A total of 92.3% of patients/guardians in the azithromycin group and 90.5% of patients/guardians in the tobramycin group rated the eye drops as comfortable on D3 (p=0.717). On D7, treatment tolerability was rated by investigators as ‘very satisfactory’ or ‘satisfactory’ for 97.1% of patients on azithromycin and 91.9% on tobramycin (p=0.076).
Discussion
Randomised controlled studies with, when possible, stratification by age group (ie, neonates, infants, children and adolescent) and designed to establish the efficacy and safety of medicinal products in the paediatric population are strongly encouraged by regulatory health authorities19. Most currently licensed topical antibiotics for bacterial conjunctivitis have been approved based on clinical studies conducted mainly in adults11, with insufficient clinical data in newborns and infants (ie, <24 months). This study has now established the efficacy and safety of azithromycin 1.5% eye drops in children with an average age of 3 years old. Patients were mainly recruited in hospital centres where usually only very young children are seen for treatment of bacterial conjunctivitis. This enabled recruitment of a large proportion (>50%) of patients younger than 24 months old compared with other studies that mostly involved children in an older age range9 ,13 ,14 ,20 ,21.
In this study, a short treatment regimen (3 days) with azithromycin 1.5% eye drops (one drop twice daily) provided a more rapid clinical cure in children with purulent bacterial conjunctivitis than did the tobramycin 0.3% eye drops regimen (every 2 h for 2 days, then four times daily for 5 days). When compared with tobramycin, efficacy of azithromycin was found to be significantly superior on D3 and non-inferior on D7. The clinical cure rates obtained for both antibiotics are very similar to those of previous studies, that is, 48% on D3 and 80% on D9 in azithromycin-treated children compared with 27% and 82% in tobramycin-treated children (6 years old on average)17 ,20.
The selection of patients with moderate to severe cardinal signs of acute conjunctivitis in this study may explain the relative high rate (71%) of positive bacterial cultures noted at baseline. However, the bacteriological profile for patients in this study is similar to the one determined in the paediatric subgroup of an earlier large randomised controlled study17 ,20 and consistent with the causative microorganisms usually found in the literature for acute conjunctivitis in young children21–23. Haemophilus influenzae was the most frequently isolated pathogen, probably owing to the high incidence of associated acute otitis media in children with bacterial conjunctivitis (reported in 20–73% of cases), as this bacteria is the predominant pathogen responsible for the conjunctivitis otitis syndrome24–26. S pneumoniae was also commonly detected in patients in this study, at a similar incidence to the Gigliotti study (14.8% vs 12.1%, respectively22). Other pathogens, such as Gram-negative bacteria other than Haemophilus, were found in a few patients. Thus, a broad-spectrum antibiotic like azithromycin is justified for use as a first-line treatment against purulent bacterial conjunctivitis in children. Moreover, the most common causative agents differ in children compared with adults, in which Staphylococcus species predominate (S epidermidis, 39%; coagulase-negative Staphylococcus, 23%; S aureus, 18%27). As most topical antibiotics are prescribed empirically without diagnostic bacteriological profiling, these findings emphasise the importance of an aetiological approach to determine the best possible initial treatment for eradication of the causative microbes, particularly in the rarely tested 0–2-year-old population.
The high rate of bacterial resolution noted in this study is consistent with the targeted efficacy of azithromycin 1.5% against the bacterial spectrum found in children. Following azithromycin treatment, the bacteriological cure rate was about 90% (D7), ranging from 76.5% to 100%, depending on the microbe. This is similar to the results previously found with both azithromycin20 and other topical ophthalmic solutions9 ,13 ,14 ,28. Azithromycin effectively eradicated all causative pathogens, including classically resistant species such as Acinetobacteria, Corynebacteria and Enterobacteria. Following azithromycin eye drop application, sustained antibiotic concentrations in tears and conjunctival cells are usually much higher than the plasma concentrations reached after oral administration of azithromycin. This could explain why even bacteria resistant to plasma concentrations of azithromycin are susceptible to azithromycin eye drop treatment (which has an antibiotic concentration several times the minimum inhibitory concentration for bacteria usually defined as resistant)27. The pharmacokinetic properties of azithromycin justify the short treatment duration of only one drop twice-daily for 3 days for a rapid antibacterial action29. The present study has confirmed that this treatment regimen, already established in adults, is also effective in the paediatric population, including children younger than 24 months old.
Combined with results from the previous study17, more than 400 children with bacterial conjunctivitis have now been treated with the azithromycin 1.5% regimen. In this study, azithromycin was found to be safe and well tolerated in children as young as a few days old, with most AEs related to ocular discomfort (burning, stinging) upon instillation. More than 90% of patients/guardians found the azithromycin eye drops comfortable, and investigators assessed the antibiotic tolerability as favourable in more than 95% of treated patients. No corneal or anterior chamber inflammation was shown at slit lamp. This also confirmed the good safety profile of azithromycin 1.5% eye drops previously established in children with trachomatous conjunctivitis30 ,31.
Patients/guardians regarded the azithromycin 1.5% regimen (one drop, morning and evening, for 3 days) a more convenient treatment, which was easier to comply with and had a significantly lower impact on daily activities in comparison to the tobramycin regimen (84.0% of patients/guardians in the azithromycin group reported their treatment as ‘never’ impacting on daily activities compared to 54.8% of patients/guardians in the tobramycin group, p<0.001; data not illustrated). Moreover, taking into consideration a similar cost of eye drops (prices in Europe were found to range between 2.7 × P and 9.2 × P for azithromycin and between 1.0 × P and 11.4 × P for tobramycin; P is the lowest price), it is likely that reduced drop instillation regimen and faster resolution of conjunctivitis would result in overall cost saving (from parental time off work, loss of earnings), but this was not directly assessed during this prospective study. A major benefit of the simple, short and effective dosing regimen for azithromycin is therefore its compatibility with real life. Such a dosage regimen is also expected to improve compliance and avoid antibiotic misuse, thereby limiting the risk of bacterial resistance developing.
In summary, azithromycin 1.5% eye drops are an effective and safe therapeutic option for purulent bacterial conjunctivitis in paediatric patients, notably in the 0–2-year-old range. Azithromycin provided a superior clinical cure rate on D3 compared with tobramycin, combined with a more convenient dosage regimen. Simplification of the therapy is a major benefit of this short-term twice daily regimen, confirmed by this study in a paediatric subgroup in whom instillation can be tricky.
Acknowledgments
The authors wish to thank Lydia Bresson, Sandrine Guyon and Nathalie Guérin who managed the study, and Hervé Chabanon for medical writing assistance.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators The investigators of the AZI Study Group are listed in the online supplementary appendix 1.
-
Contributors DB-G was the investigator coordinator of this study, participated in the design and conduct of the study, and in the review and approval of the manuscript. HN, PEB, RM, SL, LV, CS-S, DH, TK, BK-K, JM and FC were all investigators of the study, participated in the conduct of the study, and in the review and approval of the manuscript. LD and DR participated in the design and conduct of the study, and in the review and approval of the manuscript.
-
Funding The study and medical writing support were sponsored by Laboratoires Théa, Clermont-Ferrand, France. The study sponsor participated in the study design, analysis and interpretation of the data, in writing the report and in the decision to submit the paper for publication.
-
Competing interests DB-G and FC are consultants for Alcon, Allergan, Bausch & Lomb and Laboratoires Théa. However, they did not receive personal fees for this study. LD and DR are employees of Laboratoires Théa. The other authors have no conflicts of interest relevant to this article to disclose.
-
Patient consent Obtained.
-
Ethics approval Ethics committee approvals were obtained in each country prior to enrolling any patient.
-
Provenance and peer review Not commissioned; externally peer reviewed.