Article Text

Statistics from Altmetric.com
Editor,—Parvovirus B 19 is a common infection in developed countries with a seroprevalence of 40–60% in young adults.1 The commonest age of infection is 5–14 years. Clinical features of acute infection include erythema infectiosum (slapped cheek syndrome or Vth disease), arthralgia, and fever. It is usually a mild disease, but aplastic anaemia may develop in susceptible hosts and it may cause fetal loss if acquired during pregnancy. Acute infection can be accompanied by autoantibody formation including antinuclear antibodies (ANA) and rheumatoid factor (RF)2and therefore infection may share clinical and serological similarities with early rheumatoid arthritis and juvenile chronic arthritis. Uveitis in young girls usually occurs in association with early onset pauciarticular juvenile chronic arthritis which has a high frequency of ANA in the absence of RF. We report a case of uveitis in a young girl, associated with a transient ANA and RF, and serological evidence of acute parvovirus infection.
CASE REPORT
A 6 year old white girl presented with a 2 week history of a painful red left eye. She had an unaided visual acuity of 6/9 in each eye; there was a left anterior uveitis with 3+ anterior chamber cells. The uveitis was non-granulomatous with no keratic precipitates, band keratopathy, synechiae, or flare; she had a mild vitritis but no macular oedema or choroidal involvement.
Her medical history included an unspecified viral illness requiring brief hospital admission at 1 year of age from which she fully recovered. When 5 years old she developed recurrent otitis media and 6 months later underwent grommet insertion for glue ear. She developed tonsillitis and pharyngitis at 6 years associated with serological evidence of infectious mononucleosis. Her grandmother had rheumatoid arthritis, but there was no other family history of relevance.
She had a 2 year history of knee pains but had no other systemic symptoms at the onset of the uveitis.
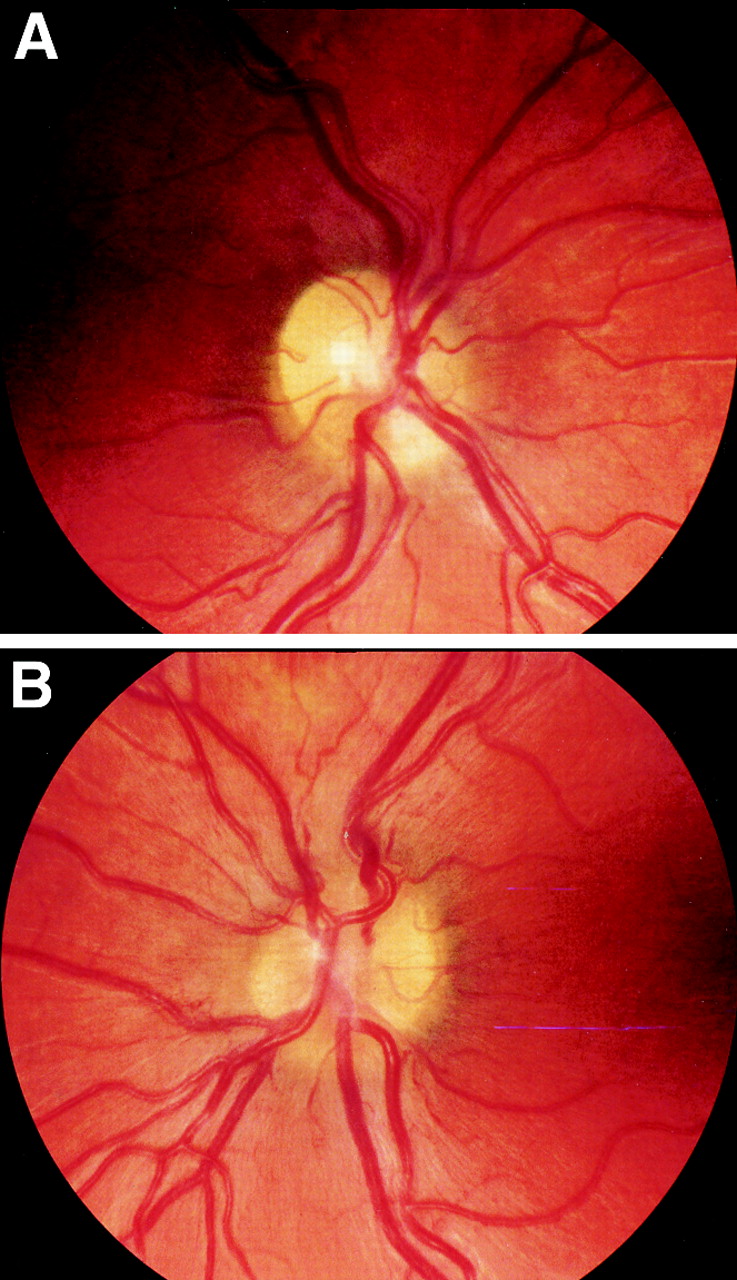
She was treated with topical steroids and cycloplegia; after 2 months she developed mild disc oedema and hypotony with intraocular pressures of 11 mm Hg right eye, 4 mm Hg left eye. Her acuity remained 6/9 in each eye, and she continued topical steroid treatment only. Ten months after onset she developed a painful right anterior uveitis, mild uveitis persisting in the left eye. Fourteen months after onset both eyes had mild panuveitis (anterior uveitis, mild vitritis, and mild disc oedema, see Fig 1); the hypotony had resolved. Visual acuity remained normal and topical steroids were withdrawn 23 months after onset when all signs of inflammation had receded. There have been no recurrences at last review 27 months after onset.
{kind=link}
Mild disc oedema, 14 months after onset of the uveitis. (A) Right eye, (B) left eye.
Repeated rheumatological examinations did not reveal any inflammatory arthritis, and her knee pains ascribed to hypermobility syndrome.
The following were normal or negative: C reactive protein (CRP), immunoglobulins, neutrophil count, liver function tests, serum angiotensin converting enzyme (ACE), anti-double stranded DNA antibodies, and titres for adenovirus, Chlamydia psittaci, hepatitis B, enterovirus, mumps, measles, herpes simplex, varicella zoster, and cytomegalovirus. There was evidence of previous infection with rubella, Epstein–Barr virus, and streptococci.
Abnormal investigations included a persistent mild lymphocytosis. The RF was positive at the onset of uveitis (24 MRF units/ml, >20 = strongly positive) but undetectable thereafter. Parvovirus IgM was positive (18 units macroelisa) at 4 months after onset, but negative thereafter (Table 1). One year after onset she had a weakly positive ANA of the nucleolar pattern.
Summary of serological abnormalities
COMMENT
Parvovirus infection has been associated with transient neurological disease including encephalitis,3 aseptic meningitis,4 neuroretinitis with disc oedema,5 ciliary ganglionitis and disc hyperaemia,6 and immune mediated inner ear disease.7 There have been no previous reports of an isolated uveitis. Our patient developed a painful chronic bilateral panuveitis and arthralgia associated with IgM antibodies to parvovirus that were detectable 3 months after onset of disease and absent thereafter. As IgM antibodies subside within 3 months of an acute infection it is likely that an acute parvovirus infection occurred at the onset of the uveitis. This allows us to postulate a causal link between the infection and the uveitis, this is not proved and another aetiological agent for the uveitis cannot be excluded. Other causes of uveitis in children include ankylosing spondylitis, trauma, toxoplasmosis, toxocariasis, pars planitis, and masquerade syndromes; Behçet's syndrome, sarcoid, Fuchs' heterochromic cyclitis, herpes simplex, and Vogt–Koyanagi–Harada are less common in younger children.
Acute parvovirus infection is known to trigger the production of autoantibodies and RF; in one study 7/53 patients developed ANA and 1/53 developed RF.2 Antibodies against immunodominant parvovirus peptides cross react with keratin, collagen type II, single strand DNA, and cardiolipin in humans; immunisation of mice with these peptides produce a similar pattern of autoantibodies.8 The seroprevalence of IgG antibodies to parvovirus has been found higher in patients with juvenile rheumatoid arthritis and rheumatoid arthritis (RA) in some studies but not in others.9 10 The arthritis associated with acute infection may only involve a few joints and most commonly involves the knee. It can therefore mimic early onset pauciarticular juvenile chronic arthritis (JCA) as well as RA.11 The differential diagnosis of acute parvovirus infection and autoimmune arthritis is sometimes only possible after exclusion of an acute parvovirus infection by examination of the changes in IgM parvovirus response.
Although most parvovirus infections resolve in a few weeks, joint symptoms may persist for several months. Recurrence of acute symptoms has also been recorded 7 years later.12 Persistent viral DNA has been fund in blood, marrow erythroid precursors, and synovium,13 but viral DNA may persist without clinical disease.10 12 13 More recently evidence has emerged of parvovirus VP-1 antigen persistence in the synovium of a high proportion (30/39) of RA patients with some markers of infectivity present in this tissue.14 It is possible that virus may persist in the eye, but the delayed onset of disease in the second eye in our case suggests that haematogenous spread was the more likely route of transmission than the activation of dormant intraocular virus.
De Boer et al 15 examined the intraocular fluids of six patients with intermediate uveitis and IgG antibodies to parvovirus in their serum. None showed evidence of intraocular antibody production, but the report did not state whether the patients ever had clinical signs of acute parvovirus infection or whether seroconversion coincided with the onset of uveitis in these patients.
Uveitis associated with ANA + JCA is almost universally a painless anterior disease without significant disc oedema or vitritis. Our case presented with a painful, red anterior uveitis later associated with a mild vitritis and disc oedema. The only other case of parvovirus uveitis described was also a bilateral panuveitis with disc involvement but was painless and caused tonic pupils.6 Calvert describes a case of unilateral neuroretinitis in a patient with AIDS that occurred during a parvovirus infection.5 Our case did not have a uveitis typical of JCA and the absence of joint inflammation or persistent JCA make it unlikely that JCA was the cause.
The incidence of uveitis in those under 10 years is low compared with adults with an age corrected incidence of 3/100 000 compared with 23/100 000 in adults (unpublished figures). A girl in the same school class as our patient developed a painful acute anterior uveitis within 1 month of the onset of disease in our index patient. She had no evidence of recent or previous parvovirus infection or any systemic inflammatory disease. It is possible that another infectious organism caused both cases.