Article Text

Abstract
Background/aims: To compare the relative risks of poly (methylmethacrylate) (PMMA) and soft acrylic (AcrySof) primary intraocular lens (IOL) implantation in paediatric cataract surgery.
Methods: A retrospective analysis of clinical data was performed on eyes of 61 infants and children who underwent cataract surgery with primary IOL implantation. Age at operation ranged from 3 weeks to 15 years. Mean follow up duration was 24.5 months (range 0.5–68 months). Factors examined included type of IOL (PMMA, acrylic), performance of a primary posterior continuous curvilinear capsulorhexis (PCCC) or capsulotomy with limited anterior vitrectomy, perioperative complications, and subsequent intervention for posterior capsule opacification (PCO). Risk factors for perioperative complications were examined with 2×2 tables to give odds ratios (OR) as measures of association. A survival analysis was performed to assess risk of subsequent intervention for PCO with different IOL types. Relative risks (hazards) and confidence intervals (CI) were calculated with Cox regression to adjust for potential confounding.
Results: Compared to acrylic, PMMA IOLs were significantly associated with perioperative complications (OR 5.2, 95% CI 1.4 to 19, p = 0.01). However, IOL and type of section were highly correlated factors, and this finding may reflect risks associated with larger scleral wounds used for PMMA IOLs. No statistically significant difference in risk of subsequent intervention for PCO was found between different IOL types. Mean times till intervention for PMMA and acrylic IOLs were 30.1 months (95% CI 22 to 38) and 19.8 months (95% CI 12 to 27) respectively (log rank test statistic 1.53, one degree of freedom, p = 0.22). At 12 months post-implant surgery, 76% (95% CI 59 to 93) of PMMA cases and 54% (95% CI 35 to 72) of acrylic cases had not required intervention for PCO; these proportions fell to 55% (95% CI 35 to 75) and 38% (95% CI 14 to 61) for PMMA and acrylic cases respectively at 2 years post-surgery. After adjustment for age at surgery, primary posterior capsulorhexis, and perioperative complications relative risk of intervention after acrylic IOL implantation was 1.6 (95% CI 0.66 to 3.9, p = 0.29).
Conclusion: Primary implantation of foldable soft acrylic IOLs in paediatric eyes may allow fewer perioperative complications than rigid PMMA IOLs. Short term safety profiles of primary implantation in paediatric cataract surgery are otherwise comparable for PMMA and soft acrylic IOLs.
- paediatric cataract
- lens implant
Statistics from Altmetric.com
Primary implantation of posterior chamber intraocular lenses (IOLs) has become an increasingly common and accepted procedure in paediatric cataract surgery, but controversy exists regarding very early implantation.1 IOL implantation in children is associated with higher perioperative complications and an increased risk of subsequent posterior capsule opacification (PCO) compared to adults.2 Primary posterior capsulotomy with limited anterior vitrectomy has been advocated to decrease PCO risk in younger eyes3 where surgical capsulotomy may be required to deal with exuberant lens fibre reproliferation.
Foldable soft acrylic IOLs have lower PCO rates than poly(methylmethacrylate) (PMMA) lenses in adult eyes,4,5 but to our knowledge only a single previous study has reported on comparative PCO rates with these lens types in infants and children.6
We report on a comparison of perioperative and subsequent complications of PMMA and foldable acrylic (AcrySof, Alcon Laboratories, Herts, UK) IOL primary implantation in paediatric eyes.
MATERIALS AND METHODS
A prospectively maintained diagnostic database was used to procure hospital records of all infants and children having primary IOL implants at Manchester Royal Eye Hospital (MREH) between March 1997 and May 2002. The MREH Department of Paediatric Ophthalmology receives specialist and optometric referrals from the North West Region of England (six million population). Referral protocols have not altered over the time of the study period. Management, surgery, and follow up assessment for each patient was either performed or supervised by one surgeon (ICL) throughout the study period.
IOL power calculations and surgical technique with PMMA implants has previously been reported.7 Scleral or limbal (with PMMA lens implantation) or clear corneal sections (with most AcrySof IOLs) were fashioned and anterior continuous curvilinear capsulorhexsis lens performed under viscoelastic. Lens material was removed using an automated irrigation/aspiration technique, and meticulous cortical clean up attempted in all cases. Posterior capsulorhexis or capsulotomy with limited anterior vitrectomy was performed in children under 4 years of age.
PMMA (Raynor 552A or Pharmacia and Upjohn 812C) or soft acrylic IOLs (AcrySof MA60 or MA30) were inserted and 10/0 Vicryl monofilament sutures placed before subconjunctival steroid and antibiotic injections. Most PMMA IOLs were implanted before 2000, and AcrySof lenses from 2000 onwards. Patients received a postoperative topical steroid/antibiotic combination for at least 3 weeks postoperatively.
Patients were monitored for postoperative and delayed complications. Significant capsule or (following primary posterior capsulorhexsis) visual axis obscuration by fibrosis and/or lens fibre proliferation was diagnosed by one surgeon (ICL).
Patients with significant PCO received YAG laser or surgical capsulotomy, depending on severity of posterior capsule thickening. Younger children had laser capsulotomy performed under general anaesthetic using a horizontally mounted delivery system; a slit lamp mounted unit and topical anaesthetic was used for older cooperative patients. Surgical capsulotomies incorporated limbal stab incisions and viscodissection of capsule leaflets away from the IOL optic. IOL tilting within the bag allowed access for a mechanical cutter to the posterior capsule area. After fashioning of a central opening smaller than optic diameter, IOLs were repositioned within the bag and incisions closed with 10-0 Vicryl. Subconjunctival steroid and antibiotic injections were given, and topical steroid/antibiotic combination continued postoperatively.
Data were recorded for interventions up to and including December 2002. Data on single eyes of individuals (all unilateral cases and right eyes of children with bilateral cataract surgery) were included in analyses to avoid correlation errors.8
Statistical analyses were performed using SPSS (Statistical Program for the Social Sciences) version 9.0. Potential risk factors for perioperative complications were examined using 2×2 tables. Log rank testing of survival distributions assessed associations between study factors and subsequent intervention for PCO. Cases contributed varying periods of event free survival time to the analysis before undergoing capsulotomy or being “censored”—that is, exiting without intervention. Cox regression was used to find relative hazards for IOL type after adjustment for potential confounding factors—age at operation, perioperative complications, and primary posterior capsulorhexis. Kaplan-Meier survival and complementary log-log curves were produced to test for proportionality of hazards. Regression models were examined for goodness of fit with tests of residuals, leverage, and interaction effects. Independent sample t tests were used to compare means between IOL groups where appropriate.
RESULTS
Eyes of 61 individual infants and children were identified and included in analysis. Four eyes received Raynor 552A IOLs, 21 Pharmacia and Upjohn 812C IOLs, 12 AcrySof MA30 and 23 MA60MA IOLs. Data on IOL type were missing for one child. Study population characteristics are given according to IOL type in table 1.
Patient characteristics by intraocular lens type
Fourteen eyes were diagnosed with autosomal dominant cataract, and four had a traumatic aetiology. Lamellar (17), posterior lenticonus (15), nuclear/embryonic (seven) and posterior subcapsular (five) cataract were the most frequent morphologies found.
Documented systemic illnesses, anomalies or syndromes included cystic fibrosis (two), asthma, galactosaemia, acute lymphoblastic leukaemia, trisomy 21, fifth finger clinodactyly, polydactyly, and autosomal dominant chromosome 16/22 translocation. Separate children had undergone previous exomphalos minor and duodenal atresia/imperforate anus repairs as neonates.
Documented ocular anomalies and syndromes included persistent hyperplastic primary vitreous (four), isolated optic nerve hypoplasia (two), Goldenhar’s syndrome, isolated aniridia, Sturge-Weber syndrome, and iris colobomata. Two children had penetrating eye injuries and two blunt trauma injuries before cataract surgery. Two other children had combined ocular and systemic findings; one child had WAGR syndrome diagnosed and another suffered asthma with an undiagnosed retinal dystrophy, anterior segment dysgenesis and retinopathy of prematurity.
Perioperative complications in PMMA cases included posterior capsular breach (one), anterior capsulorhexis tear out with vitreous to the wound (one), IOL optic displacement anterior to the capsule (one), iris prolapse (one), pupil capture (one), and fibrinous uveitis (five). Three AcrySof cases had posterior capsular rupture noted at the time of surgery. Pupil peaking secondary to a vitreous strand was first noted at 1 month postoperatively in another AcrySof case where no intraoperative posterior capsule breach or zonulysis was documented. Two of the posterior capsule breaches (one acrylic and one PMMA case) occurred in eyes with posterior lenticonus cataract. No cases of endophthalmitis occurred. Table 2 displays unadjusted odds ratios of complications for study factors.
Associations between study factors and perioperative complication*
Mean follow up duration was 35.3 months (range 13–68 months) for PMMA cases and 17.4 months (range 0.5–47 months) for acrylic implanted eyes. Fifteen of 25 PMMA cases, and 16 of 35 eyes implanted with acrylic IOLs, underwent at least one subsequent laser or surgical capsulotomy during totals of 594 months and 392 months of at-risk follow up respectively. Twenty four children were followed without subsequent intervention until the end of the study period. Two children were previously discharged to follow up elsewhere, each after 6 months. Three failed to attend subsequent clinic appointments after follow up of 2 weeks, 6 weeks, and 26 months.
Kaplan-Meier survival curves by IOL type, age group, primary posterior capsulotomy/capsulorhexis, and perioperative complication are shown in figures 1–4 with test statistics given. At 12 months post-implant surgery, 76% (95% CI 59 to 93) of PMMA cases and 54% (95% CI 35 to 72) of acrylic cases had not required intervention for PCO. Non-intervention rates at 18 and 24 months for PMMA eyes were 60% and 55%, and for acrylic 49% and 38% respectively. Complications were found to significantly increase risk of capsulotomy when early follow up was weighted (Breslow test statistic 4.82, p = 0.03) although the overall log rank statistic was not significant (log rank statistic 1.73, p = 0.19). Age group was found not to significantly affect risk (log rank statistic 0.75, p = 0.69), but a trend for posterior capsulorhexis to protect against PCO was suggested (log rank statistic 2.36, p = 0.12).
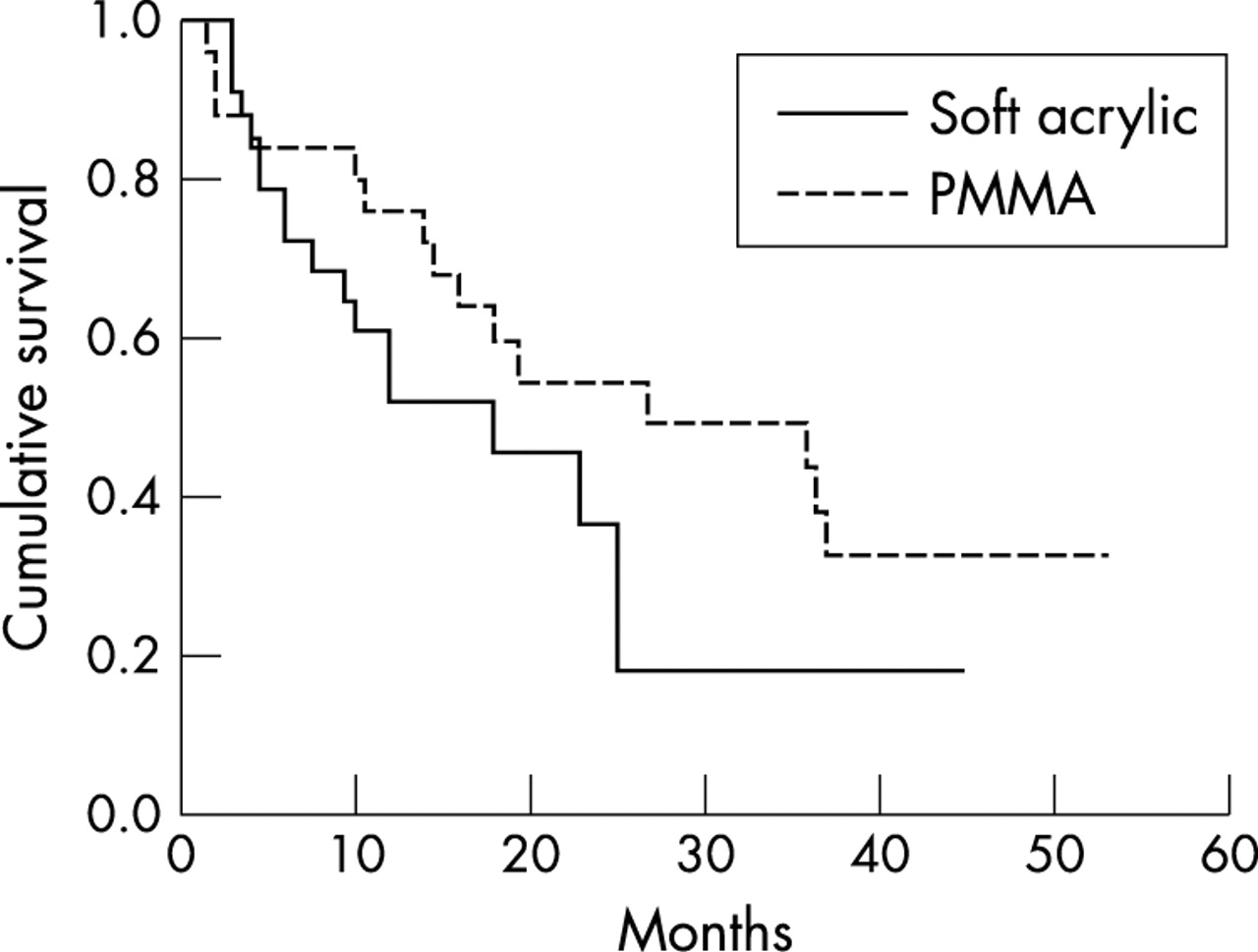
Survival functions by IOL type. Log rank statistic 1.53, p = 0.23; Breslow statistic 1.02, p = 0.32.

Survival functions by age group. Log rank statistic 0.75, p = 0.69; Breslow statistic 0.33, p = 0.85.
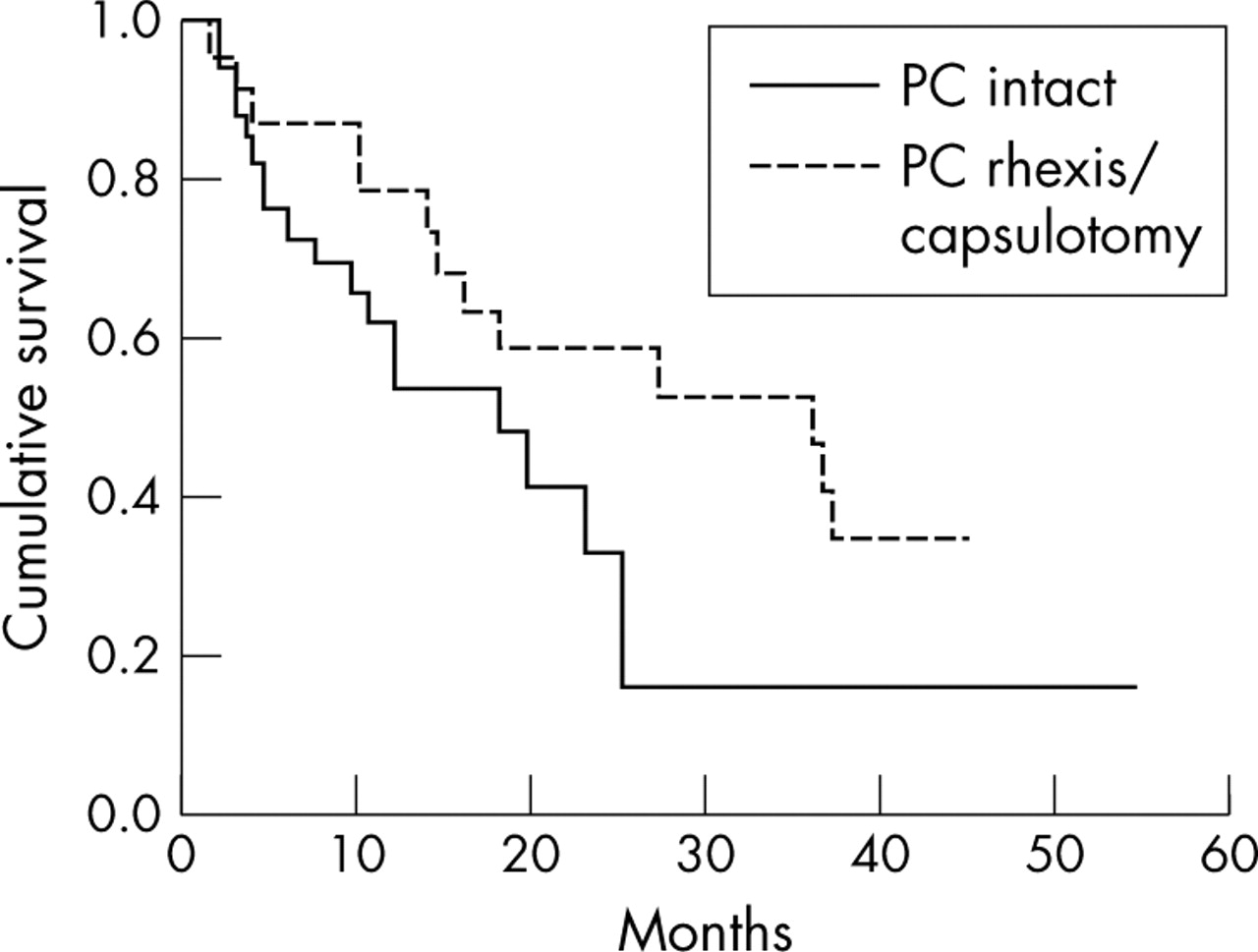
Survival functions by primary posterior rhexis/capsulotomy status. Log rank statistic 2.36, p = 0.12; Breslow statistic 1.77, p = 0.18.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Survival functions by perioperative complications status. Log rank statistic 1.73, p = 0.19; Breslow statistic 4.82, p = 0.03.
Relative risks (“hazards”) of subsequent capsulotomy are given in table 3 for IOL type and other study factors. Systemic or ocular anomalies were both non-significant predictors of subsequent intervention for PCO. After adjustment for age at operation, perioperative complications and primary posterior capsulorhexis, no statistically significant difference in risk of subsequent capsulotomy was found between IOL types (p = 0.29). Perioperative complications increased risk of intervention (relative risk 3.3, 95% CI 1.3 to 8.2, p = 0.01) while a statistical trend for a protective effect of primary posterior capsulorhexis was found (p = 0.08).
Relative risks (“hazards”) of capsulotomy after intraocular lens implant*
No children were diagnosed with retinal detachment during follow up. Pseudophakic glaucoma leading to trabeculectomy was diagnosed in one child who received an acrylic implant. No other children received glaucoma medication and intraocular (Pulsair) pressures (IOP) at last follow up were not statistically different between IOL groups; PMMA (n = 25) and acrylic (n = 33) mean IOPs were 13.5 mm Hg and 12.3 mm Hg respectively (p = 0.23).
DISCUSSION
Compared with PMMA IOLs, foldable soft acrylic lens implants allow smaller wounds and have lower rates of PCO in adults.4 Soft acrylic IOLs have been implanted in paediatric eyes since at least 1995,6 but to our knowledge, there are few reports comparing perioperative and longer term safety of PMMA and AcrySof IOL in children.6
In the MREH series, perioperative complications were more common in cases of PMMA implant, in younger children, and with performance of primary posterior capsulorhexis or capsulotomy. However, interpretation of these associations is problematic because of correlations between study factors in the data. All PMMA cases had scleral or limbal sections performed whereas 28 of 32 AcrySof cases had clear corneal sections. This high correlation existing between IOL and section type means that the effects of these factors on risk of perioperative complications cannot be separated. Similarly, fewer correlations between IOL type, patient age, and posterior capsule management again make separation of the individual effect of these factors difficult. The apparent effect of IOL type may in parts reflect increased technical difficulty associated with large incision size and insertion of a rigid lens in smaller less rigid eyes. Most PMMA cases were also performed historically earlier, and higher rates of complications in this cohort may partly reflect a surgical learning curve.9
The risk of intervention for PCO was found not to significantly differ between IOL types. Apart from IOL material type, lens (“square edge”) optic design has been found to affect PCO risk in adult eyes.5 All acrylic IOLs were of one design in our cohort and the lens design effect was not separable from that of material type. Study power limitations related to the sample size means a true difference in risk of PCO requiring intervention cannot be excluded.
In our case series, age at operation was found not to independently predict subsequent intervention for PCO. Plager et al10 also found no difference in opacification rates for children 18 months to 18 years at IOL implantation. However, high PCO rates in infants have been frequently reported.2,11 With only 13 eyes implanted under 12 months available for analysis, our findings may reflect low study power and failure to detect a real effect.
A trend was found for a protective effect of primary posterior capsulotomy or capsulorhexis. O’Keefe et al11 also found anterior vitrectomy appeared to reduce reoperation rates in infants aged less than 1 year. The same authors have also compared PCO rates following posterior capsulorhexis performed with or without anterior vitrectomy.12 Analysis of a possible additional effect of vitrectomy was not performed in our study because of small case numbers in the subgroup of patients receiving only capsulorhexis.
When early follow up was weighted, perioperative complications were found to increase risk for subsequent capsulotomy. A putative mechanism for this finding may lie in the presence of fibrin/vitreous scaffolds, incomplete cortical clear up, humoral factors, and inflammatory mediators combining to promote lens epithelial proliferation.
A recent article has also reported comparable rates of laser capsulotomy for PCO between AcrySof and PMMA IOLs in children.6 Wilson et al found 45% of Acrysof v 50% of PMMA cases had capsulotomies. Mean time from surgery was 18.6 months for AcrySof and 18.3 months for PMMA. However, follow up times were markedly shorter for AcrySof cases (mean 65 v 137 weeks, p<0.001) and capsulotomies would be reasonably expected beyond this time, from the above data. Patient withdrawal from, or incomplete, follow up before development of significant PCO may bias findings in this situation. χ2 and t tests, used for statistical comparison of capsulotomy rates and time to capsulotomy, respectively, may not deal optimally with differing durations of follow up between groups.
A survival analysis of PCO risk with different IOLs was performed in our study. This method allows for variable follow up and enables adjustment for potential confounders. Assumptions underlying survival analysis include constant recruitment methods and diagnostic criteria.13 In our study, referral basis and patterns were unchanged during the period of entry. All patient care, from initial assessment to decision for PCO intervention, was determined by the same experienced consultant surgeon throughout the entire study period. Another assumption of survival analysis is that of non-informative censoring—that is, leaving a study and suffering an outcome are independent events. Though not testable from the data, censoring of cases was non-informative to our knowledge.
After decades of implantation in adult eyes, PMMA has a demonstrated long term biocompatibility. The long term biocompatibility of foldable acrylic is not known currently. However, in the context of adult cataract surgery, foldable soft acrylic IOLs have obvious advantages over rigid PMMA in allowing smaller wound sizes and less postoperative intervention for PCO. Our findings suggest comparable safety profiles exist for paediatric eyes receiving these as primary implants in the short term.
Acknowledgments
The authors would like to thank Dr Steve Roberts for advice regarding statistical analyses and Ms Sarah Davies for assisting with data collection.
REFERENCES
Linked Articles
- BJO at a glance